










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versión impresa ISSN 2341-4545
GE Port J Gastroenterol vol.27 no.1 Lisboa feb. 2020
https://doi.org/10.1159/000497387
CLINICAL CASE STUDY
A Rare Pancreatic Tail Metastasis from Squamous Cell Lung Carcinoma Diagnosed by EUS-FNB and a Small Review of the Literature
Um caso raro de metástase na cauda do pâncreas de carcinoma de células escamosas do pulmão por EUSFNB e uma pequena revisão da literatura
Ioannis Stoupisa, Evangelos Voudoukisb, Emmanouil Mastorakisc, Georgios Kazamiasc, Panagiotis Ieromonachoud, Charalampos Pappase
aDepartment of Internal Medicine, Division of Internal Oncology, Rethymnon General Hospital, Rethymnon, Greece;bDepartment of Gastroenterology, Venizeleion General Hospital of Heraklion, Rethymnon, Greece; cDepartment of Cytopathology, Venizeleion General Hospital of Heraklion, Rethymnon, Greece; dDepartment of Histopathology, Venizeleion General Hospital of Heraklion, Rethymnon, Greece; ePneumonology Department, Rethymnon General Hospital, Rethymnon, Greece
* Corresponding author.
ABSTRACT
Differential diagnosis of pancreatic lesions is really challenging, especially when the patient is diagnosed with primary cancer at another site. In this case report, we managed to histologically confirm pancreatic metastasis from squamous cell lung carcinoma, which is a very rare entity, using endoscopic ultrasound fine needle biopsy.
Keywords: Lung cancer, Squamous cell, Pancreatic metastasis,·EUS-FNB
RESUMO
O diagnóstico diferencial de lesões pancreáticas é desafiante, especialmente quando o doente é diagnosticado com cancro primário noutro local. Neste caso clínico foi possível confirmar histologicamente o diagnóstico de metástase pancreática de carcinoma de células escamosas do pulmão, que se trata de uma entidade muito rara, através de punção com agulha fina ecoguiada por ecoendoscopia.
Palavras-chave: Cancro pulmão de células escamosas, Metástase pancreática, EUS-FNB
Introduction
Secondary lesions in the pancreas are uncommon and difficult to discriminate from a primary pancreatic cancer. An accurate diagnosis can provide the appropriate treatment to the patient. In this case, the patient had synchronous pancreatic metastasis originating from a primary non-small cell lung cancer, and the pancreatic tumor was diagnosed using endoscopic ultrasound-guided fine needle biopsy (EUS-FNB). EUS has proven to be a safe and optimal diagnosing tool for evaluating pancreatic tumors [1].
Case Report
A 60-year-old woman, a current smoker with > 50 pack/years, was admitted to the General Hospital of Rethymnon on February 2018 due to fatigue, cough, and hemoptysis. She reported loss of appetite and a 10-kg weight loss during the past 6 months. Her blood count was low with iron deficiency anemia (Hgb 9.2 g/dL), but the rest of the blood tests were within normal limits. The tumor marker results were as follows (CEA 1.5 μg/L, Ca19-9 22.4 U/mL, and Ca15-3 30.6 U/mL).
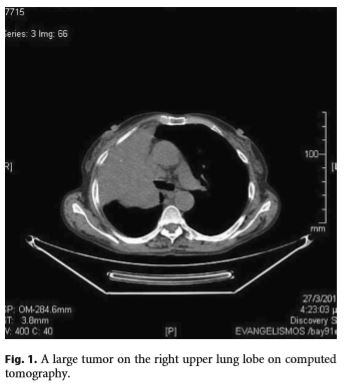
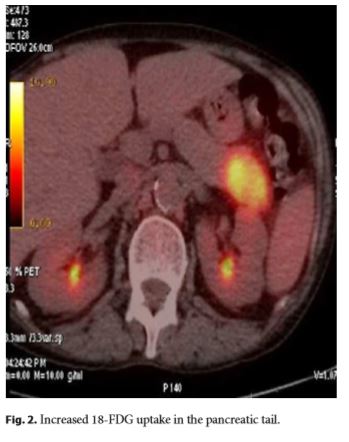
During the medical workup, a chest X-ray depicted a large mass on the right upper lung lobe, which was confirmed on contrastenhanced chest computed tomography (CT) scan (Fig. 1). CT scan also revealed 2 pathologically enlarged right hilar lymph nodes. Subsequent bronchoscopy revealed obstruction of the right superior lobar bronchus from a mass, and histopathology reported squamous cell carcinoma (SCC) of the lung. The physician ordered a positron emission tomography/CT, which showed increased 2-deoxy-2-[F-18]fluoro-D-glucose uptake in the right lung and pancreatic tail (Fig. 2).
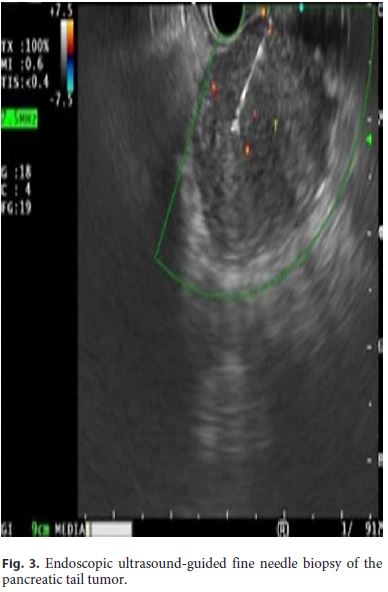
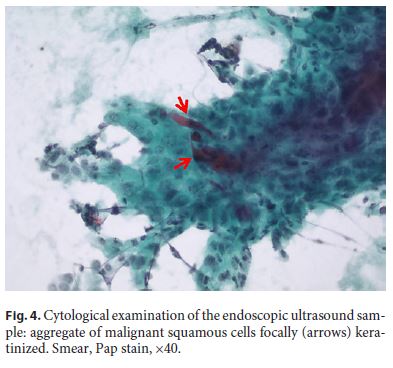
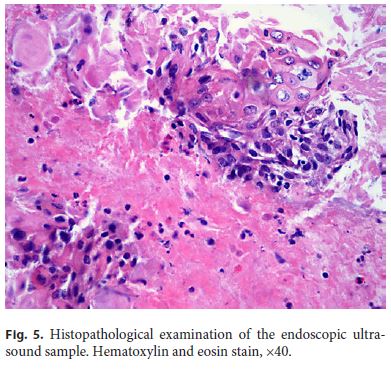
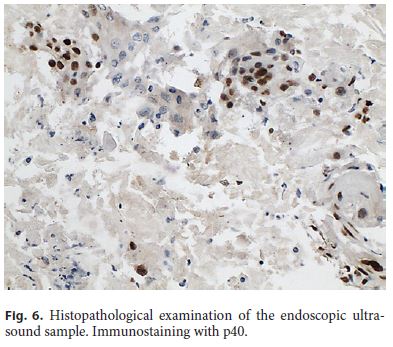
Subsequently, the patient was referred for EUS, and a hypoechoic 4.5-cm pancreatic-tail round mass with slightly irregular borders was identified. The lesion was clearly separated from the left adrenal gland and the kidney, and EUS-FNB was performed using a 22-gauge needle (Acquire, Boston Scientific, Natick, MA, USA) (Fig. 3). Cytology stain slides revealed atypical squamous cells suggestive of the diagnosis of SCC (Fig. 4). Needle core fragments were collected separately and sent for histopathological evaluation, which revealed keratin debris, apoptotic keratinocytes, and few solid aggregates of atypical cells featuring focally intercellular bridges and intracellular keratinization (Fig. 5). Positive immunostaining with p40 supports the squamous phenotype (Fig. 6). Thus, this was diagnosed as a metastatic pancreatic tumor from lung cancer.
A programmed cell death-1 (PD-L1) biomarker test (22C3 PharmDx DAKOTM kit) was done using paraffin-embedded slides of the primary tumor which showed a Tumor Proportion Score of 5.801/6.408 (90.5%). After that, the patient was treated with the anti-PD-L1 antibody pembrolizumab, and she is still alive after 7 cycles of therapy without having any adverse events and with stable tumor burden after her last CT scans.
Discussion
The prevalence of pancreatic metastases, in large autopsy series of metastatic disease, has been described to range from 1.6 to 11% [2]. Metastatic tumors in the pancreas are uncommon neoplasms accounting for less than 3% of solid pancreatic lesions and are mainly related to advanced disease [3, 4]. Most common metastatic malignancies in the pancreas are those of the kidney, lung, melanoma, and breast. Lung cancers have the tendency to metastasize to adrenal glands, liver, brain, and bones and less frequently to other sites [5]. Regarding lung-related pancreatic metastases, the frequency is mostly related to the histological type, with small cell carcinoma being the most common, followed by adenocarcinoma, large cell carcinoma, and lastly SCC, being the least frequent, occurring only in 1.1% of these tumors [4]. To our knowledge, only 4 cases of metastatic lung SCC in the pancreas have been reported worldwide, but 3 of them were lesions identified several months after the diagnosis and treatment of lung cancer and were not a concomitant diagnosis of primary and metastatic site as in our case [3, 4, 6, 7]. Pancreatic SCC could be of primary origin, but this constitutes a rather questionable entity, as the pancreas is devoid of squamous cells, and, thus, in such cases, an extensive workup should be performed to rule out possible metastasis from the lungs, esophagus, and cervix [8].
EUS is now considered the gold standard examination for diagnosing and differentiating pancreatic tumors [1]. Over the last few years, a new trend has been developed for solid abdominal and especially pancreatic lesions regarding the type of tissue acquisition needle used. FNB needles have gained ground as they are now considered delivering a more accurate diagnostic sample and with fewer passes needed compared to fine aspiration needles in EUS [9–11].
There are no defined criteria for the management of metastases in the pancreas, but the prognosis is poor and, often, a more conservative approach is preferred. In conclusion, when faced with pancreatic solid lesions, physicians should always keep in mind the likelihood of metastasis from tumors with unusual site and histology. EUS with FNB remains the optimal diagnostic tool for these kinds of lesions.
References
1 Hasan MK, Hawes RH. EUS-guided FNA of solid pancreas tumors. Gastrointest Endosc Clin N Am. 2012 Apr;22(2):155–67. [ Links ]
2 Adsay NV, Andea A, Basturk O, Kilinc N, Nassar H, Cheng JD. Secondary tumors of the pancreas: an analysis of a surgical and autopsy database and review of the literature. Virchows Arch. 2004 Jun;444(6):527–35. [ Links ]
3 Ishikawa T, Hirooka Y, Teman CJ, Goto H, Belletrutti PJ. An Unusual Case of Pancreatic Metastasis from Squamous Cell Carcinoma of the Lung Diagnosed by EUS-Guided Fine Needle Biopsy. Case Rep Gastrointest Med. 2017;2017:3212056. [ Links ]
4 Liratzopoulos N, Efremidou EI, Papageorgiou MS, Romanidis K, Minopoulos GJ, Manolas KJ. Extrahepatic biliary obstruction due to a solitary pancreatic metastasis of squamous cell lung carcinoma. Case report. J Gastrointestin Liver Dis. 2006 Mar;15(1):73–5. [ Links ]
5 Kurihara N, Saito H, Nanjo H, Konno H, Minamiya Y. Pancreatic metastasis from nonsmall-cell lung cancer diagnosed using endoscopic ultrasound-guided fine needle aspiration biopsy: A case report. Turk J Gastroenterol. 2017 Nov;28(6):502–4. [ Links ]
6 Sharma A, Alfa-Wali M, Rodriguez-Justo M, Polychronis A. Squamous cell carcinoma of pancreas: an unusual site of relapse from early-stage lung cancer: 12-month postsurgery. BMJ Case Rep. 2013 Apr;(apr22 1):2013. [ Links ]
7 Mockli GC, Silversmith M. Squamous cell carcinoma of the lung metastatic to the pancreas: diagnosis by fine-needle aspiration biopsy. Diagn Cytopathol. 1997 Mar;16(3):287–8. [ Links ]
8 Brijbassie A, Stelow E, Shami VM. Squamous Cell Carcinoma of the Pancreas: A Case Report and Review of Literature. Gastroenterol Res. 2014 Aug;7(3-4):102–4. [ Links ]
9 Tian L, Tang AL, Zhang L, Liu XW, Li JB, Wang F, et al. Evaluation of 22G fine-needle aspiration (FNA) versus fine-needle biopsy (FNB) for endoscopic ultrasound-guided sampling of pancreatic lesions: a prospective comparison study. Surg Endosc. 2018 Aug;32(8):3533–9. [ Links ]
10 Cheng B, Zhang Y, Chen Q, Sun B, Deng Z, Shan H, et al. Analysis of Fine-Needle Biopsy vs Fine-Needle Aspiration in Diagnosis of Pancreatic and Abdominal Masses: A Prospective, Multicenter, Randomized Controlled Trial. Clin Gastroenterol Hepatol. 2018 Aug;16(8):1314–21. [ Links ]
11 Lee YN, Moon JH, Kim HK, Choi HJ, Choi MH, Kim DC, et al. Core biopsy needle versus standard aspiration needle for endoscopic ultrasound-guided sampling of solid pancreatic masses: a randomized parallel-group study. Endoscopy. 2014 Dec;46(12):1056–62. [ Links ]
Statement of Ethics
We state that the subject of this case has given her written informed consent to publish her case (including publication of images).
Disclosure Statement
There are no conflicts of interest.
Funding Sources
There is no financial support and sponsorship for this article.
* Corresponding author.
Ioannis Stoupis
Department of Internal Medicine, Division of Internal Oncology
General Hospital of Rethymnon, Trandalidou Street 17
GR–74100 Rethymnon, Crete (Greece)
E-Mail stigiannis@gmail.com
Received: December 9, 2018; Accepted after revision: January 29, 2019
Author Contributions
Ioannis Stoupis: manuscript writer, medical oncologist in charge of making the treatment plan for the patient. Evangelos Voudoukis: manuscript writer, has done the EUS-FNB to the patient. Emmanouil Mastorakis: manuscript writer, contributed to immunohistochemistry and histological diagnoses of the EUSFNB specimen. Georgios Kazamias: manuscript writer, contributed to cytological diagnoses of the EUS-FNB specimen. Panagiotis Ieromonachou: manuscript writer, contributed to immunohistochemistry and histological diagnoses of the EUS-FNB specimen. Charalampos Pappas: manuscript writer, contributed to bronchoscopy, staging procedures, and diagnoses of the primary tumor.

