










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
Print version ISSN 2341-4545
GE Port J Gastroenterol vol.27 no.1 Lisboa Feb. 2020
https://doi.org/10.1159/000499979
CLINICAL CASE STUDY
In the Beginning … It was Already the End
No princípio ... Já foi o fim
Claudia Janeiro, Rita Santos, João Teixeira, Pedro Mesquita, Rosário Eça, Luis Vale
Centro Hospitalar Universitário de Lisboa Central, Hospital de Santo António dos Capuchos, Serviço de Medicina 2.1, Lisbon, Portugal
* Corresponding author.
ABSTRACT
Sometimes, the presentation of some diseases can be fulminating. The authors present the case of a 51-year- old male brought to the emergency department visibly drunk and complaining of abdominal pain. Immediately, the diagnosis of hemorrhagic shock due to an accentuated drop of the hemoglobin level was made. After stabilization, he underwent a computed tomography of the abdomen, revealing a hepatocellular carcinoma with rupture of the Glisson capsule and massive intraperitoneal hemorrhage. With this case, the authors want to bring attention to a rare first presentation of hepatocellular carcinoma with a catastrophic result.
Keywords: Abdominal pain, Alcohol, Chemoembolization, Cirrhosis, Liver cancer
RESUMO
Por vezes a apresentação de algumas patologias pode ser fulminante. Os autores apresentam o caso de um doente de 51 anos que foi trazido ao Serviço de Urgência em etilismo agudo com dor abdominal mas rapidamente foi constatado choque com queda acentuada da hemoglobina confirmando-se choque hemorrágico. Após estabilização realizou Tomografia Computadorizada abdominal constatando-se carcinoma hepatocelular com rotura da cápsula de gleason e hemorragia intra-peritoneal maciça. Com este caso os autores pretendem chamar a atenção para uma apresentação inicial rara de carcinoma hepatocelular mas cujo resultado é catastrófico.
Palavras-chave: Dor abdominal, Álcool, Quimioembolização, Cirrose, Carcinoma hepatocelular
Introduction
Malignant tumors of the liver and biliary tract, to which hepatocellular carcinoma belong, represent a mortality rate of 1.0% in Portugal, corresponding to 1.3% of deaths in male patients and 0,6% of deaths in female patients (total of 1,036 deaths) according to the last reported data in 2013 [1]. The average age of death was 71.3 years in total, 69.8 years for males, and 74.8 years for females [1]. Worldwide, hepatocellular carcinoma is the sixth most common cancer, being responsible for 600,000 deaths annually [2].
The risk factors identified for cancer development are infection with hepatitis B virus [3], hepatitis C virus [4], alcohol [5], morbid obesity [6], diabetes and, as a consequence, fatty liver [6]. Other, less common diseases such as hemochromatosis [7] are also known risk factors. The authors present this case not only for its rarity but also for the diagnostic challenge that it may represent.
Clinical Case
A male Caucasian patient of 51 years, owner of a restaurant, was directly admitted to the emergency room for a 1-h history of altered mental status, decreased skin perfusion, and sweating. He was still arousable, with an ethylic breath and complaining of intense abdominal pain. Initially, after a spike in tension of 160/70 mm Hg, he rapidly evolved to shock with persistent hypotension and tachycardia. After a fluid challenge, only partial recovery of blood pressure was seen. An arterial blood sample was taken at admission, revealing metabolic acidosis with hyperlactacidemia. The values were: pH 7.129; pCO2 35 mm Hg; pO2 82 mm Hg; Lact 15 mmol/L, and bicarb of 11.7 mmol/L.
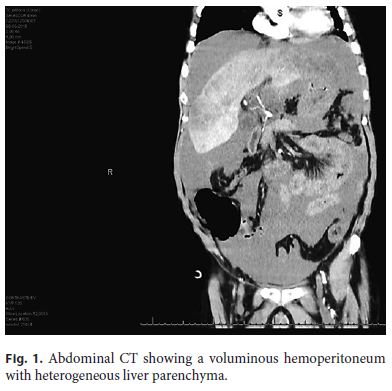
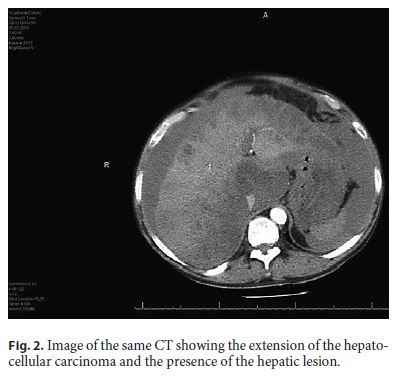
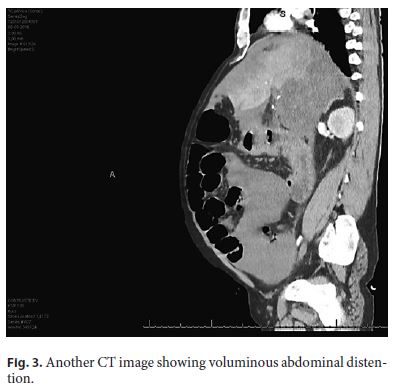
Clinically, there was a slight improvement in the neurologic state with recovery of consciousness but with a visible increase in abdominal size even though the patient stopped complaining about abdominal pain. A second arterial blood sample was taken with a slight decrease of the lactate level to 13 mmol/L, still in metabolic acidosis, but the thing that caught our attention was a drop in the hemoglobin level from 9.4 g/dL to 6.2 g/dL, leading to the diagnosis of hemorrhagic shock. After exclusion of gastric hemorrhage and blood transfusions, the patient underwent a computed tomography (CT) of the abdomen (Fig. 1, Fig. 2, Fig. 3) that revealed a massive hemoperitoneum and heterogeneous liver suggestive of hepatocellular carcinoma. In liver segments II, III, VI and VII, there was capsular indefinition in relation to the rupture caused by the liver cancer and consequently massive hemoperitoneum. Several enlarged ganglia intra-abdominally and micronodularity of the great omentum were suggestive of peritoneal carcinomatosis. No intra-abdominal free air was present.
Probably at the point in time when the rupture of the Glisson capsule occurred, the abdominal pain improved due to a decrease in the intrahepatic pressure consequent to the decrease in distention of the Glisson capsule. Laboratory results were an alcohol level of 360 mg/L, a hemoglobin level of 9.5 g/dL (sample taken at admission) with macrocytosis, low platelets of 69,000, spontaneous INR 1.43, fibrinogen level of 1.8 g/L, aspartate transaminase 107 U/L, alanine transaminase 26 U/L, gamma-glutamyl transpeptidase 210 U/L, and a normal bilirubin level.
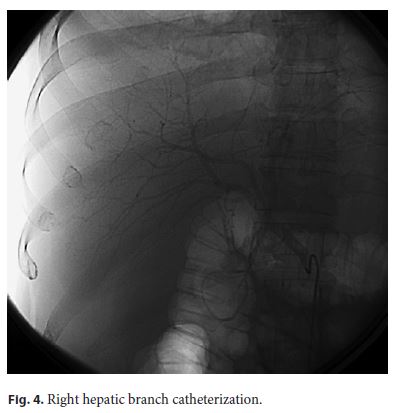
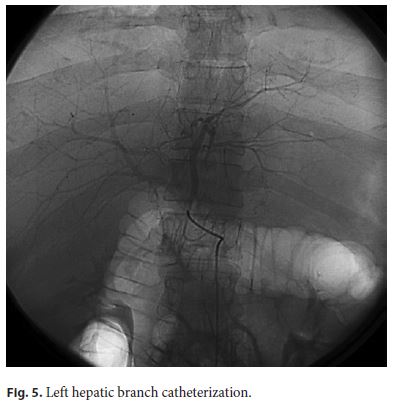
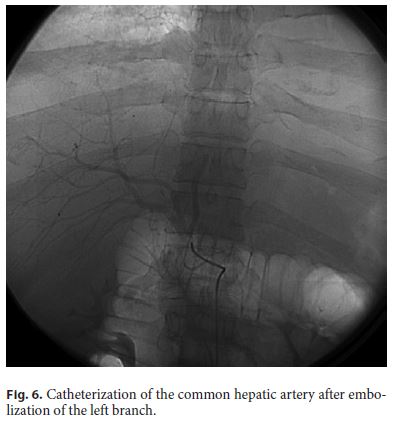
He was admitted to the surgical ward and submitted to angiography. After visualization of the celiac trunk, common hepatic artery and left and right branches as well as a voluminous left hepatic lesion with hypervascularization were seen without evidence of active hemorrhage. Transarterial chemoembolization of the left branch of the hepatic artery was performed as it was the suspected to be the source of hemorrhage seen on the CT scan (Fig. 4, Fig. 5, Fig. 6).
In spite of best care, the patient died on the second day after admission. It is important to notice that he had already been admitted to this same hospital for 7 days 9 months before for a first episode of ascites due to liver disease treated by another medical team. Sparse body hair as well as superficial venous abdominal circulation were seen. At that time, hepatic ultrasound was performed confirming the presence of ascites, enlarged liver but with a regular contour, and no focal lesions. No changes in the hepatic vessels with normal and welldirected flow. His serum albumin level was 33 and 17.5 g/L in ascitic fluid with a serum-ascites albumin gradient of 15.5 g/L, suggestive of portal hypertension. No neoplastic cells or bacteria where isolated. He was oriented to an outpatient hepatology clinic that he never visited, and he kept his alcoholic drinking habits.
Serologic studies for hepatitis A, B, and C virus as well as HIV were performed, all with negative results. Alpha-fetoprotein was 2.39 ng/mL (normal range < 8.78).
At that time, alcohol consumption was estimated around 200 g/day, and he had a smoking history of 49 pack-years.
Discussion
Although rarely, hepatocellular carcinoma can manifest as severe intra-abdominal hemorrhage with hemodynamic instability. According to published series, this form of presentation is seen in < 5% of the cases in the western countries [8–11] but is more elevated in Asian countries such as Japan (2.9–14%) [12], Thailand (12.4%) [13], and Hong Kong (14.5%) [14]. Although the exact mechanism is not known yet, subcapsular location, tumor necrosis, portal hypertension, rapid growth, and an increase of the venous pressure by vascular invasion of the tumor are factors frequently involved in rupture. In addition, the size and involvement of the left lobe are considered an increased risk because tumoral growth is more probable to cause distention and consequent rupture of the Glisson capsule [15]. With this case, we would also like to bring attention to the fact the patient presented with alcohol intoxication. This should be correctly evaluated, as such patients sometimes present with serious medical conditions that require immediate treatment. In patients with chronic alcohol intake who have this kind of presentation, gastric or variceal hemorrhage should also be considered, as they are more frequent causes of bleeding. Since we excluded upper gastrointestinal tract bleeding, CT was fundamental for the diagnosis that otherwise would only have been possible by surgical laparotomy/laparoscopy.
This is an initial, rare, and fulminating presentation of hepatocellular carcinoma with rapid growth and rupture of the Glisson capsule of the liver, leading to massive intraperitoneal hemorrhage with shock. Despite being submitted to transarterial chemoembolization of the main hepatic lesion, the prognosis was poor, and despite best treatment, the patient died about 48 h after admission.
References
1 Instituto Nacional de Estatística. Causas de morte 2013. Available from: https://www.ine.pt. [ Links ]
2 Venook AP, Papandreou C, Furuse J, de Guevara LL. The incidence and epidemiology of hepatocellular carcinoma: a global and regional perspective. Oncologist. 2010;15 Suppl 4:5–13. [ Links ]
3 Cougot D, Neuveut C, Buendia MA. HBV induced carcinogenesis. J Clin Virol. 2005 Dec;34 Suppl 1:S75–8. [ Links ]
4 Maki A, Kono H, Gupta M, Asakawa M, Suzuki T, Matsuda M, et al. Predictive power of biomarkers of oxidative stress and inflammation in patients with hepatitis C virus-associated hepatocellular carcinoma. Ann Surg Oncol. 2007 Mar;14(3):1182–90. [ Links ]
5 Clemens DL, Forman A, Jerrells TR, Sorrell MF, Tuma DJ. Relationship between acetaldehyde levels and cell survival in ethanol-metabolizing hepatoma cells. Hepatology. 2002 May;35(5):1196–204. [ Links ]
6 Starley BQ, Calcagno CJ, Harrison SA. Nonalcoholic fatty liver disease and hepatocellular carcinoma: a weighty connection. Hepatology. 2010 May;51(5):1820–32. [ Links ]
7 Niederau C, Fischer R, Sonnenberg A, Stremmel W, Trampisch HJ, Strohmeyer G. Survival and causes of death in cirrhotic and in noncirrhotic patients with primary hemochromatosis. N Engl J Med. 1985 Nov;313(20):1256–62. [ Links ]
8 Calvet X, Bruix J, Bru C, Ginés P, Vilana R, Solé M, et al. Natural history of hepatocellular carcinoma in Spain. Five year's experience in 249 cases. J Hepatol. 1990 May;10(3):311–7. [ Links ]
9 Akriviadis EA. Hemoperitoneum in patients with ascites. Am J Gastroenterol. 1997 Apr;92(4):567–75. [ Links ]
10 Castells L, Vargas V, Comas P, García Sureda D, Vidal X, Esteban R, et al. [Hepatocellular carcinoma: clinical aspects, diagnosis, and survival in 140 cases]. Med Clin (Barc). 1993 Mar;100(12):441–6. [ Links ]
11 Vivarelli M, Cavallari A, Bellusci R, De Raffele E, Nardo B, Gozzetti G. Ruptured hepatocellular carcinoma: an important cause of spontaneous haemoperitoneum in Italy. Eur J Surg. 1995 Dec;161(12):881–6. [ Links ]
12 Hirai K, Kawazoe Y, Yamashita K, Kumagai M, Nagata K, Kawaguchi S, et al. Transcatheter arterial embolization for spontaneous rupture of hepatocellular carcinoma. Am J Gastroenterol. 1986 Apr;81(4):275–9. [ Links ]
13 Chearanai O, Plengvanit U, Asavanich C, Damrongsak D, Sindhvananda K, Boonyapisit S. Spontaneous rupture of primary hepatoma: report of 63 cases with particular reference to the pathogenesis and rationale treatment by hepatic artery ligation. Cancer. 1983 Apr;51(8):1532–6. [ Links ]
14 Ong GB, Taw JL. Spontaneous rupture of hepatocellular carcinoma. BMJ. 1972 Oct;4(5833):146–9. [ Links ]
15 Lai EC, Wu KM, Choi TK, Fan ST, Wong J. Spontaneous ruptured hepatocellular carcinoma. An appraisal of surgical treatment. Ann Surg. 1989 Jul;210(1):24–8. [ Links ]
Statement of Ethics
The authors have no ethical conflicts to disclose.
Disclosure Statement
The authors have no conflicts of interest to declare.
* Corresponding author.
Luis Vale
Serviço de Medicina 2.1, Hospital de Santo António dos Capuchos
Alameda de Santo António dos Capuchos
PT–1169-050 Lisbon (Portugal)
E-Mail Luisfvale_238@hotmail.com
Received: January 15, 2019; Accepted after revision: February 26, 2019
Author Contributions
The authors would like to thank Dr. Tiago Bilhim for the pictures of the transarterial procedure.

