










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.27 no.2 Lisboa abr. 2020
https://doi.org/10.1159/000500145
ENDOSCOPIC SNAPSHOT
Endoscopic Palliation of Hilar Cholangiocarcinoma: Usefulness of Selective Occlusion of One Intrahepatic Duct
Paliação Endoscópica do Colangiocarcinoma Hilar: Utilidade da Oclusão Seletiva de Um Ducto Intrahepático
João Fernandesa,b, Tarcísio Araújoa, Jorge Canenac, Luís Lopesa,d,e
aGastroenterology Department, Hospital Santa Luzia, Viana do Castelo, Portugal; bGastroenterology Department, Centro Hospitalar Cova da Beira EPE, Covilhã, Portugal; cNova Medical School/FCML, Universidade Nova de Lisboa, Lisbon, Portugal; dLife and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, Braga, Portugal; eICVS/3Bs – PT Government Associate Laboratory, Braga/Guimarães, Portugal
* Corresponding author.
Keywords: Hilar cholangiocarcinoma, Endoscopic retrograde cholangiopancreatography, Malignant biliary stenosis, Palliative biliary drainage
Palavras-Chave: Colangiocarcinoma hilar, CPRE, Estenose biliar maligna, Drenagem biliar paliativa
Endoscopic retrograde cholangiopancreatography with stent placement for palliative biliary drainage is a common strategy used in the management of patients with unresectable hilar cholangiocarcinomas [1, 2].
Selective placement of two guidewires, one in the right intrahepatic duct (RIHD) and the other in the left hepatic duct (LIHD), is an essential prerequisite for bilateral stenting. However, the insertion of the second guidewire to the contralateral intrahepatic duct can be extremely difficult in some patients, even after using multiple maneuvers, using different types of catheters and guidewires [3, 4].
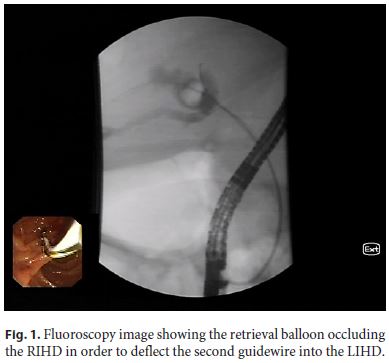
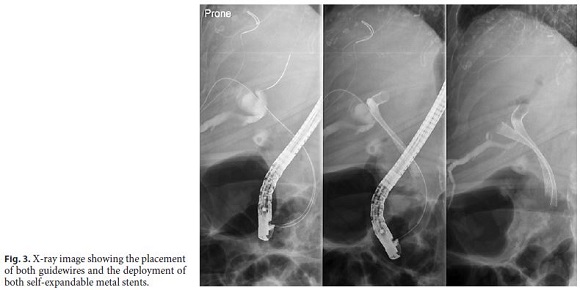
In this video (online suppl. Video 1; see www.karger.com/doi/10.1159/000500145 for all online suppl. material), we demonstrate a technique to overcome the inability to direct the second guidewire to the contralateral intrahepatic duct. We describe an 85-year-old man, with a type II hilar cholangiocarcinoma, referred to our department for palliative bilateral stenting. After swiftly passing the first guidewire to the right lobe, we faced unexpected difficulties in directing the second guidewire to the dilated LIHD. Several maneuvers were attempted, including the use of angled-tip and small caliber hydrophilic wires, but all resulted invariably in the cannulation of the right system. In order to overcome this difficulty, we introduced a 15-mm retrieval balloon into the dilated RIHD; the balloon was inflated immediately proximal to the hepatic bifurcation, blocking the access to the RIHD. Subsequently, a second guidewire was inserted alongside the balloon catheter, across the hilar stricture and easily deflected off the inflated balloon into the LIHD (Fig. 1). Two self-expandable metal stents were successfully deployed (Fig. 2, 3).

To the best of our knowledge, there are no multimedia reports on this technical tip to facilitate the passage of a second guidewire to the opposite intrahepatic duct, which was first reported by Husain et al. [5]. The use of this technical maneuver could be a very useful tool for increasing the success of bilateral stenting in patients with hilar cholangiocarcinoma.
References
1 Dumonceau JM, Tringali A, Blero D, Devière J, Laugiers R, Heresbach D, et al.; European Society of Gastrointestinal Endoscopy. Biliary stenting: indications, choice of stents and results: European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline. Endoscopy. 2012 Mar;44(3):277–98.
2 Larghi A, Tringali A, Lecca PG, Giordano M, Costamagna G. Management of hilar biliary strictures. Am J Gastroenterol. 2008 Feb;103(2):458–73.
3 Kim JY, Kang DH, Choi CW, Kim HW, Park SB, Kim DU. Selective intrahepatic duct cannulation by using a triple-lumen catheter for endoscopic bilateral stenting in hilar cholangiocarcinoma. Gastrointest Endosc. 2010 Jul;72(1):192–8.
4 Gulati A, Thakkar P, Thakkar S. Endoscopic management of hilar stricture. Tech Gastrointest Endosc. 2016;18(2):67–74.
5 Husain A, Debold C, Edmundowicz SA, Jonnalagadda SS. Directed balloon-assisted guidewire access into intrahepatic ducts. Gastrointest Endosc. 2001 Jul;54(1):118–9.
Statement of Ethics
This study did not require informed consent nor review/approval by the appropriate ethics committee.
Disclosure Statement
The authors declare no conflict of interest.
* Corresponding author.
João Fernandes
Department of Gastroenterology, Hospital de Santa Luzia
Unidade Local de Saúde do Alto Minho, Estrada de Santa Luzia
PT–4901-858 Viana do Castelo (Portugal)
E-Mail jotillfernandes@hotmail.com
Received: January 23, 2019; Accepted after revision: April 1, 2019
Author Contributions
J.F. and L.L. wrote the manuscript. T.A. and J.C. were responsible for the revision of its contents.

