










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
Print version ISSN 2341-4545
GE Port J Gastroenterol vol.27 no.6 Lisboa Dec. 2020
https://doi.org/10.1159/000507204
ENDOSCOPIC SNAPSHOT
Downside-Up Retrograde Dilation for “Lost Cap” Retrieval as a Signature Complication of Esophageal BougieCap Dilation
Dilatação retrógrada invertida para recuperação de uma “cap perdida” como complicação sinalizadora de uma dilatação esofágica por BougieCap
Vincent Zimmera,b
aDepartment of Medicine, Marienhausklinik St. Josef Kohlhof, Neunkirchen, Germany; bDepartment of Medicine II, Saarland University Medical Center, Saarland University, Homburg, Germany
* Corresponding author.
Keywords: Esophageal stricture, Dilation, Bougienage, BougieCap, Retrieval
Palavras-Chave: Estenose esofágica, Dilatação, Bougienage, BougieCap, Recuperação
A novel device designated BougieCap (Ovesco, Tübingen, Germany) has been marketed for endoscopic treatment of esophageal strictures under both visual and haptic control [1]. A recently published prospective multicenter study on the utility and complications in its mainstay indication has reported high rates of endoscopic and clinical success. On the downside, loss of the BougieCap with subsequent passage into the stool has been documented in 2/50 individuals, such that “the lost cap” may be considered a signature complication due to insufficient attachment by circular taping and/or, albeit unproven, stricture length and tightness [2]. While no clinical consequences from the lost caps were reported, potential clinical and/or medicolegal implications may arise reminiscent of small-bowel capsule retention [3].
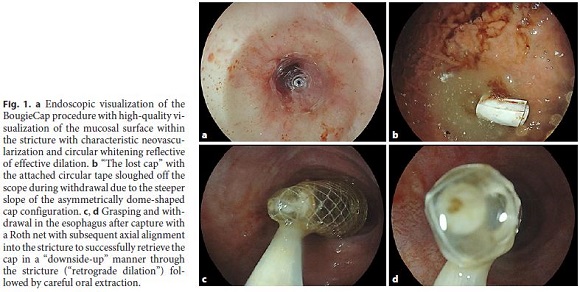
Against this background, I would like to present the first report of successful lost BougieCap retrieval through a tight radiation-induced upper esophageal stricture. We performed BougieCap dilation in a 78-year-old male patient with high-grade dysphagia due to a complex upper esophageal stricture precluding standard scope passage after definitive radiochemotherapy for squamous cell carcinoma. In a first session, dilation with a 7- and 10-mm BougieCap was performed with guidewire assistance. In another session 4 days apart, 12-, 14-, and 16-mm caps were used without using a guidewire. Highquality mucosal characterization within the stricture through the BougieCap in tight mucosal contact clearly revealed radiation-induced neovascularization without evidence of mucosal relapse (Fig. 1a). However, given the steeper slope at the back of the dome-shaped cap, sloughing off the endoscope occurred with immediate gastric migration (Fig. 1b). Retrieval of the cap through the stricture was successful after grasping it with a Roth net in full axial alignment in an “downside-up” manner and careful extraction through the stricture, thus, performing “retrograde dilation” (Fig. 1c, d). Bleeding and/or perforation could be excluded after retrieval by repeat endoscopy.
References
1 Cortez-Pinto J, Mão de Ferro S, Dias Pereira A. Use of the novel BougieCap in the treatment of esophageal peptic stricture. Endoscopy. 2019 Sep;51(9):E251–2.
2 Walter B, Schmidbaur S, Rahman I, Albers D, Schumacher B, Meining A. The BougieCap - a new method for endoscopic treatment of complex benign esophageal stenosis: results from a multicenter study. Endoscopy. 2019 Sep;51(9):866–70.
3 Lee HS, Lim YJ, Kim KO, Jang HJ, Chun J, Jeon SR, et al.; Research Group for Capsule Endoscopy/Small Bowel Endoscopy. Outcomes and Management Strategies for Capsule Retention: A Korean Capsule Endoscopy Nationwide Database Registry Study. Dig Dis Sci. 2019 Nov;64(11):3240–6.
Statement of Ethics
Patient consent has been obtained.
Disclosure Statement
The author declares that he has no conflicts of interest to disclose.
* Corresponding author.
Dr. Vincent Zimmer
Department of Medicine, Marienhausklinik St. Josef Kohlhof
Klinikweg 1–5
DE–66539 Neunkirchen (Germany)
Received: November 13, 2019; Accepted: January 20, 2020

