











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkEndoscopic treatment of pancreatic pseudocyst has experienced great progress in recent years, and it is becoming the first-line treatment in many cases [1, 2]. Nowadays, endoscopic ultrasound-guided drainage has played a central role as a minimally invasive technique [3, 4]. The transpapillary approach could be an alternative choice for endoscopic treatment of pancreatic pseudocyst, if transmural drainage is not feasible due to distance or is contraindicated [5]. This report describes an unusual complication of transpapillary stenting in the management of pancreatic pseudocyst.
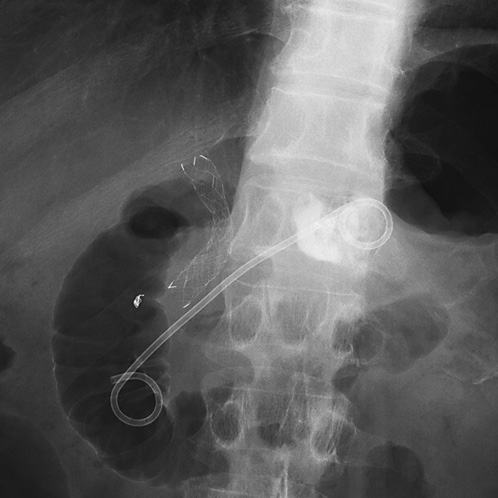
A 69-year-old man, who had been diagnosed with locally advanced pancreatic ductal adenocarcinoma with marked atrophy of upstream pancreas, presented with slight epigastric discomfort and fever. Computed tomography revealed a 3.5-cm pseudocyst associated with the pancreatic body carcinoma and engorgement of collateral veins (Fig. 1), and we considered that the pseudocyst might be the cause of symptoms. Although the patient had received intravenous ceftriaxone for 3 days, he showed no sign of improvement. Taking the risk of bleeding from the collateral veins into account, we performed endoscopic transpapillary drainage of the pseudocyst instead of endoscopic ultrasound-guided drainage. A 7-Fr, 10-cm double pigtail stent, which was considered to be associated with less migration and perforation, was successfully placed transpapillary (Fig. 2), and purulent discharge came out through the stent. The patient’s symptoms improved immediately after the drainage, and he was discharged without any sequelae. Nineteen days later, upper gastrointestinal endoscopy was performed to investigate the cause of anemia. Unexpectedly, a pigtail was found to protrude into the gastric lumen with formation of a fistula between the pseudocyst and the stomach (Fig. 3). Transient bleeding from the fistula was presumed to be the cause of anemia; however, no further development of anemia was observed. Although the double pigtail stent was not removed, no problem related to the stent was observed until he died from the pancreatic ductal adenocarcinoma 5 months later.

Fig. 1 Computed tomography showed a pancreatic pseudocyst associated with locally advanced pancreatic body carcinoma.

We have considered that the pigtail in the duodenum prevents migration and that the pigtail in the pseudocyst avoids the risk of perforation. Although uncommon, clinicians should consider the potential risk associated with the pigtail when using a double pigtail stent for transpapillary drainage of pancreatic pseudocyst.

