











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
A 61-year-old man presented to the emergency department with hematemesis. The patient referred epigastric pain, anorexia, and vomits for the past 3 days. He had a medical history of dyslipidemia and chronic venous insufficiency under treatment with bioflavonoids and a statin. Physical examination was unremarkable. Laboratorial analysis revealed a serum hemoglobin of 9.6 g/dL (normal range 13-18 g/dL). Fluids and a bolus of esomeprazole were administered, and the patient was submitted to an esophagogastroscopy (Fig. 1). Esophagogastroscopy revealed a 5-cm spheric subepithelial lesion with central ulceration and pulsatile bleeding in the posterior wall of the gastric corpus (Fig. 1). Endoscopic treatment was performed with adrenalin injection in the ulcer margins and application of 4 clips on the vessel, which controlled the bleeding. Bite-on-bite biopsies of the ulcer borders were performed due to the suggestive features of a ruptured gastrointestinal stromal tumor (GIST) [1]. Due to the impossibility of complete closure of the ulcer and doubts if the bleeding completely stopped, hemospray® was applied over the lesion (Fig. 2). The biopsy samples were insufficient for histological characterization. A CT scan revealed a 5-cm nodular lesion with heterogeneous contrast enhancement in the posterior wall of the stomach without evidence of invasion of adjacent structures or metastatic disease. The differential diagnosis should be made with other potentially malignant subepithelial lesions of the stomach, namely, leiomyoma, glomus tumor, or neuroendocrine tumor. Nevertheless, the alternative diagnoses were less likely due to the ulceration, the location of the lesion, and the heterogeneous contrast enhancement in the CT scan [1-3].
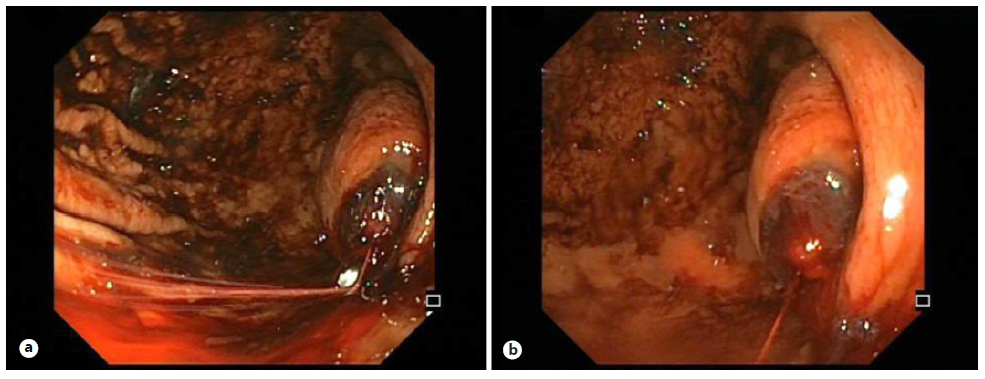
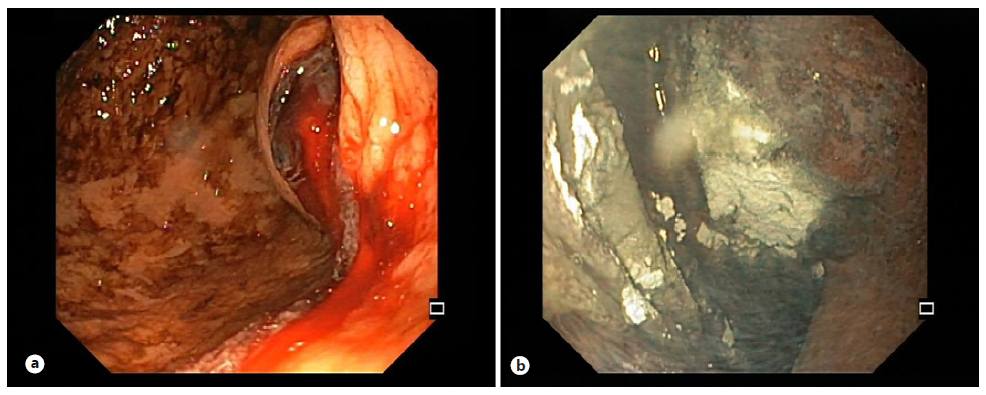
Fig. 2 Endoscopic view of the gastric corpus after adrenalin injection in the bleeding lesion (a) and at the end of the endoscopic treatment (b).
The patient was submitted to an elective partial gastrectomy. The histological exam confirmed the diagnosis of a GIST with positive immunohistochemical staining for CD34, CD117, and DOG1 with preserved SDHB expression (stage pT2 G1 N0 R0) [4, 5]. One year after the diagnosis, the patient has no evidence of disease. This endoscopic snapshot illustrates a typical presentation of a large gastric GIST with massive luminal bleeding [5]. Endoscopic treatment was performed with success as a bridge to surgery [5].

