










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkPortuguese Journal of Public Health
versión impresa ISSN 2504-3137versión On-line ISSN 2504-3145
Port J Public Health vol.35 no.2 Lisboa 2017
https://doi.org/10.1159/000481967
RESEARCH ARTICLE
Self-Reports of Health before and during. Imprisonment in Female Inmates
Auto-relatos sobre a sua saúde de reclusas antes e durante a prisão
Joana Alves, Ângela Costa Maia
School of Psychology, University of Minho, Braga, Portugal
ABSTRACT
The health of female inmates has been described as more vulnerable than that of detained male and the overall female population. The purpose of this study is to describe health behaviors, history of diseases, health complaints, and health status of 232 incarcerated women. The women reported risk behaviors and unexpected health surveillance before their imprisonment. In prison, their tobacco use increased, drug consumption decreased and high rates of diseases, use of medicines, health complaints, and poor health status were found. The women’s perceptions of their current health, compared with the time period before prison, revealed different types of impact, with one-third reporting health improvements. These data suggest that women prisoners’ health and the prison’s impact on their health must be better studied in order to enhance the health intervention programs during imprisonment.
Keywords: Female inmates, Risk behaviors, Health surveillance, Health complaints, Health status
RESUMO
A saúde das reclusas tem vindo a ser descrita como mais vulnerável do que a dos homens reclusos e do que a da população feminina em geral. O objetivo deste estudo é descrever comportamentos relacionados com a saúde, história de doenças, queixas de saúde e estado geral de saúde de 232 mulheres detidas. As participantes relataram comportamentos de risco e uma inesperada vigilância de saúde prévios à reclusão. Na prisão, o uso de tabaco aumentou e o consumo de drogas diminuiu; revelou-se também a elevada prevalência de doenças, de consumo de medicamentos e de queixas de saúde, assim como o estado geral de saúde debilitado. A percepção das reclusas sobre a sua saúde atual, em comparação com o período de tempo anterior à reclusão, revelou diferentes tipos de impacto, com um terço das mulheres a relatar melhoria do estado de saúde. Estes dados sugerem a importância de aprofundar o estudo da saúde das mulheres reclusas e o impacto da prisão no estado de saúde, a fim de aprimorar os programas de intervenção em saúde durante a reclusão.
Palavras Chave: Reclusas, Comportamentos de risco, Vigilância de saúde, Queixas de saúde, Estado de saúde
Introduction
The inmate population has been the subject of a number of studies that demonstrate specific characteristics, regarding their familial, social, demographic, economic, educational and behavioral backgrounds, which make them highly vulnerable 1. This vulnerability is reflected on several domains, but it has a special impact on health. Growing up in adverse environments, with less access to education, health services, and job opportunities, facilitates the adoption of risk behaviors and the development of adverse experiences that could result in poor physical and mental conditions 2. As a consequence, inmates usually arrive in prison presenting a debilitated health condition, including a higher prevalence of substance abuse, mental disorders, and infectious and chronic diseases [3 , 4].
If health status in an imprisonment environment is worth highlighting, the health of the female prison population requires even more dedication from both the scientific community and current health policies. Although gender is one of the most significant demographic predictors of health status 3, it has been greatly neglected in studies on inmate populations. Because of this gap, many authors have focused on health conditions in prison environments and concluded that female inmates, when compared with detained men or with the overall female population, experience higher levels of vulnerability and have higher rates of health risk behaviors and health problems, before and during imprisonment [4 - 8].
Although investigation of detained women has been increasing in recent years, a number of gaps remain in the characterization of the general health status 9, sexual behaviors, women’s specific health needs 6, and prevalence of chronic diseases 10. As stated recently by Moschetti et al. 11, descriptive studies are needed to raise awareness of the specific health issues of detained women and to support the decision-making about the most appropriated health services in female prisons.
Therefore, this article intends to characterize the health of a sample of female inmates in 4 categories: health behaviors, history of health and disease treatment, health complaints, and general health status. The study of these categories paves the way for addressing the following objectives: (a) identifying health risk behaviors: tobacco, alcohol, drug consumption, and sexual behavior before and during imprisonment; (b) monitoring self-destructive behaviors: number of suicide attempts during lifetime and self-harm behaviors during imprisonment; (c) evaluating health surveillance, that is, the use of health services before imprisonment; (d) accessing lifetime histories of sexual and reproductive health; (e) accessing lifetime histories of infectious, contagious and chronic diseases; (f) monitoring the consumption of medicines during imprisonment; (g) accessing physical and psychological health complaints during imprisonment; (h) characterizing general health statuses and individual self-perceptions of health during imprisonment, and comparing these with the individual self-perceptions of health before imprisonment.
Once the study has been carried out in two Portuguese female prison establishments, it is relevant to clarify that, in Portugal, the access to health care by the prisoners should follow the European recommendations, considering the prisoner as a citizen, with full right of access to health care. The Portuguese law states that a prisoner has the right to access the National Health Services under identical conditions to those guaranteed to all citizens; even more, prison establishments must be prepared with adequate facilities and equipment to the needs of daily life of prisoners, namely the health needs. Therefore, each female prison has its own health services including nurses, a general practitioner (GP), a psychiatrist, a gynecologist, an infectologist, a psychologist, and a dentist. This health care facility operates 24 h/day with a nurse present at all times. Immediately after admission, all new detainees are submitted to a triage process by a primary health care nurse (within the first 24 h) and by a GP (within the first 72 h) in order to identify any possible health problem.
Two hundred and thirty-two inmates in Portuguese women’s prisons participated in this study. Of the 596 women who were detained in the only two special feminine prisons during the recruitment period, 4 were released before research staff could approach them. Of the women who were screened, 71 did not meet the following inclusion criteria: ability to communicate in Portuguese and not being in an inpatient clinic condition due to unstable physical or mental health. Of the remaining 521, 250 (48%) women were randomly selected. Two hundred and thirty-two women agreed to participate in the study. The remaining 18 (7.2%) declined or decided to interrupt their participation during data collection. The response rate was 92.8%.
The most common reason for detention ( n = 131; 56.5%) was substance-related crimes. Just over half ( n = 122; 53.3%) of the women had been detained for 12 months or more, and most of them ( n = 150; 65.2%) had already been sentenced. The mean sentence length was 79.06 months (with a minimum of 6 months and a maximum of 324 months). A large majority ( n = 179; 77.8%) had been detained for the first time and, among the recidivists, the highest number of re-offenses was 4.
Demographic and Juridical Questionnaire. The demographic measures comprised age, nationality, ethnicity, education, employment, motherhood, and marital status. The juridical measures were prison, the type of crime, the duration of imprisonment, whether they had been sentenced or were on remand, the length of the sentence, and the number of times the women had been arrested.
Risk Behavior and Health History Assessment Survey. A risk behavior and health history assessment survey was created for this study. It contained questions on health risk behaviors (tobacco, alcohol and substance consumption along with sexual behavior before and during imprisonment); self-destructive behaviors (number of suicide attempts during lifetime and self-harm behaviors during imprisonment); health surveillance (previous contact with health care services); sexual and reproductive life history; and life history of infectious, contagious and chronic diseases. Participants were also asked whether they had taken any type of medication during their imprisonment.
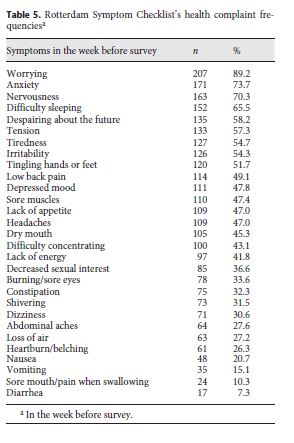
Rotterdam Symptom Checklist 12 . This questionnaire evaluated recent health complaints and featured a list of 29 symptoms divided into 2 categories: physical and psychological symptoms. The item responses were given on 4-point Likert-type scales: “not at all,” “a few times,” “sometimes,” and “very often.” However, for data analysis purposes, we dichotomized these variables and combined “not at all” and “a few times” as 0 and “sometimes” and “very often” as 1. The internal consistency reliability coefficient of the scale scored on the Portuguese sample was very good (Cronbach’s alpha of 0.91) 13.
Short-Form Health Survey (SF-12) 14. SF-12 measures subjective health status in 8 health aspects and results in a physical component summary (PCS – subscales of physical function, physical performance, pain, and general health) and a mental component summary (MCS – subscales of vitality, social function, emotional performance, and mental health). Through a specific algorithm, we obtained scores ranging from 0 to 100, where 100 corresponded to the best perception of health. The SF-12 score was produced using the Health Outcomes Scoring Software 4.0 (QualityMetric Incorporated, New York, NY, USA). Regarding the internal consistency of the Portuguese version, the Cronbach alphas were 0.79 for the PCS and 0.81 for the MCS. Sensibility tests have shown that the SF-12 appears to be a valid measurement of health status 15.
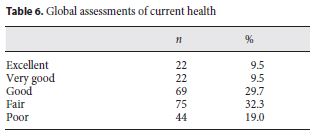
Overall Health and Health prior to Imprisonment. Two items were created to measure overall health and health prior to imprisonment. On the first item, inmates were asked about their current health: “Overall, how would you describe your health?” This question had 5 possible answers: “excellent,” “very good,” “good,” “fair,” or “poor.” The second item asked inmates to compare their current health with their health prior to being incarcerated (“Compared with the time before you were arrested, how would you describe your current health?”). The question had the following 5 possibilities for answers: “much better,” “better,” “approximately the same,” “worse,” or “much worse.”
After approval from the Ethics Committee of the General Directorate of Prison Services, the data collection was scheduled with the directing boards of each prison involved in this study. Data were collected individually by trained researchers who were not part of the prison personnel, allowing inmates to share information in an environment of confidentiality. At the beginning of each interview, the aims of the study were explained, and data were collected after obtaining the informed consent.
Data analysis was conducted using the statistics software IBM SPSS version 20. The means and standard deviations of the interval variables and the frequencies and percentages of the nominal variables were calculated in order to perform the descriptive analysis necessary to accomplish the aims of this study. For the report of percentages, we considered the value of valid percentage to better express the differences amount of missing values for each variable. The medians for the two main components of the SF-12 were also calculated in order to compare these results with the normative values for the Portuguese population 13. For this comparison, the one-sample Wilcoxon signed-rank test was used.
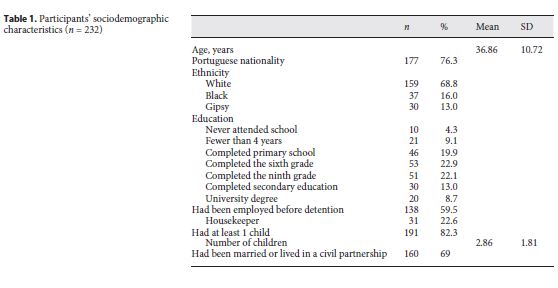
A summary of the participants’ sociodemographic characteristics is presented in table 1 .
Regarding tobacco consumption, 56.9% ( n = 132) of the participants were smokers, and the mean age for initiating smoking was 16.73 years (SD = 6.50), ranging from 9 to 43 years. Among these inmates who smoke, 62.9% ( n = 83) reported smoking more since being detained, with a mean of 15 cigarettes a day (SD = 9.89).
Most participants ( n = 188; 81%) declared they had consumed alcohol at least once. Among these, 14% ( n = 26) affirmed that their consumption was problematic, and 6.5% ( n = 12) said they had at some point been dependent on this substance. During the 6 months prior to imprisonment, alcohol consumption was considered predominantly occasional ( n = 134; 71.3%). Since their imprisonment, only 17.2% ( n = 39) of inmates mentioned alcohol consumption; among these, 86.8% ( n = 33) had consumed small portions with the consent of prison staff, and 13.2% ( n = 5) reported they had consumed alcohol during temporary leaves.
Thirty-five percent ( n = 80) of the participants reported having consumed illegal substances, and among those, 58.8% ( n = 47) considered their illegal substance use problematic. Furthermore, 57.5% ( n = 46) reported being addicted. The mean age of initial consumption was 19.86 years (SD = 7.90), with cannabis ( n = 48; 60%), cocaine ( n = 50; 62.5%), heroin ( n = 30; 37.5%), and methadone ( n = 21; 26.3%) being the most used substances prior to imprisonment. Among all inmates who reported hav ing consumed these substances, 27.5% ( n = 22) have done it intravenously (6 on their last day before being arrested, 1 during the week before, another during the month before, and 14 more than 2 months before). The average initial age of intravenous consumption was 24.86 years (SD = 9.02). Sixteen inmates (6.9%) said they had consumed drugs during imprisonment, with cannabis being the most used substance. None of the inmates answered positively to intravenous drug consumption.
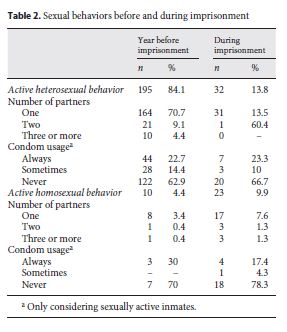
The majority of participants ( n = 195; 84.1%) reported active heterosexual behavior during the year prior to the imprisonment. Among these, only 22.7% ( n = 44) reported always using a condom. During the detention period, only 13.8% ( n = 32) revealed active heterosexual behavior, within which 23.3% ( n = 7) had always used a condom. Active homosexual behavior in the year prior to the imprisonment was reported by 4.4% ( n = 10) of the women, from which only 3 (30%) had always used a condom. Inside the prison establishment, 9.9% ( n = 23) of the participants reported active homosexual behavior, within which 17.4% ( n = 4) had always used a condom. table 2 shows detailed data on the inmates’ sexual behaviors before and during imprisonment.
Only 1 of the participants reported having been paid with money, goods or drugs for sex during imprisonment, although 23 (10%) said they had been paid with money, goods or drugs for the same purpose at some point in their lives.
Regarding suicide, 31% ( n = 72) reported at least 1 attempt; the mean number of suicide attempts was 2.3 (SD = 1.46), and the mean age of occurrence was 29 years (SD = 9.97). Within this group, 43.1% ( n = 31) said they had attempted suicide at least once while they were already in prison.
Self-harming behaviors during the month that preceded the interview, i.e., when inmates were already in prison, were reported by 10 (4.3%) participants, and in each case, the detainees reported having injured themselves to address feelings of rage, tension, anxiety, or depression. Six of these had received medical attention and/or psychological support in the prison’s medical facilities immediately after the self-harm episode.
Among the participants in this study, 90.9% ( n = 211) were registered at a primary health care center with a GP, and among those, 73.9% ( n = 156) had visited their GPs at least once in the last 6 months before imprisonment, 41.7% ( n = 108) had had an emergency hospitalization, and 19.6% ( n = 44) were being followed by a psychiatrist.
Most inmates ( n = 205; 88.4%) had been pregnant at least once. Regarding menstruation, 82.8% ( n = 192) were still menstruating at the time of the study and 45.8% ( n = 88) reported they had menstruation-related problems. The most referenced problems were irregular menstrual cycles ( n = 58, 65.9%) and very heavy bleeding ( n = 29, 33%). Before imprisonment, 51.3% ( n = 119) of inmates had been using some form of birth control methods, with oral contraceptive pills being the most common method ( n = 72; 50.7%), followed by condoms ( n = 35, 18.3%). Twenty-two percent ( n = 51) of inmates stated they were still using a contraceptive method during imprisonment, with oral birth control pills being again the most common method ( n = 22; 38.6%). Sixteen (6.9%) participants said they had been treated at least once for a sexually transmissible disease.
The number of participants receiving, at least once in their life, diagnostic tests for infectious diseases and the prevalence of these diseases are shown in table 3 .
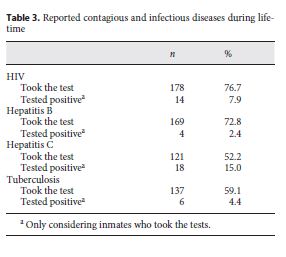
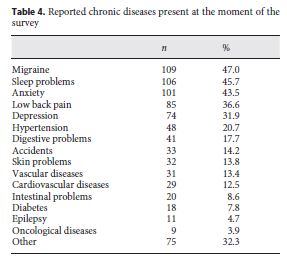
Table 4 shows the data on reported chronic diseases present at the moment of the survey, from the most to the least frequent.
Regarding pharmaceutical drugs consumed during imprisonment, 71.6% ( n = 166) of inmates reported they were taking a prescribed drug.
Table 5 lists the health complaints, including the results from the Rotterdam Symptom Checklist, that inmates had experienced during the week before the survey, by order and frequency. The most reported health complaints were essentially psychological, with worrying, anxiety, nervousness, difficulty sleeping, despair about the future, tension, tiredness, and irritability reported by more than half of participants.
The global results from the SF-12 showed that the PCS scores varied between 15.15 and 71.82, with a mean of 49.93 (SD = 10.40) and a median of 52.37 (IQR = 14.46), and the MCS scores varied between 8.89 and 64.38, with a mean of 39.84 (SD = 12.84) and a median of 40.26 (IQR = 20.66). The comparison between this study’s median PCS and MCS values and those of the reference population, using the one-sample Wilcoxon signed rank test, showed a significant difference ( z = –13.202, p = 0.05; z = –13.205, p = 0.05). Female prisoners had lower scores on both summaries, indicating poorer physical and mental health.
Table 6 shows how inmates evaluated their health at the time of the survey. In regard to their global assessment of health, in comparison with health before imprisonment, 33.2% ( n = 138) of participants said they had felt a positive shift, describing their health at the time of the survey as much better (16.8%; n = 39) or better (16.4% n = 38) than the period before prison; another 26.3% ( n = 61) reported no change, considering that their health had remained roughly the same, and 40.5% ( n = 94) reported a negative change, assessing their health statuses as worse (22.8%, n = 53) or much worse (17.7%, n = 41).
This study covered a comprehensive range of health and health behaviors in female inmates, before and during imprisonment. There is a consensus in the literature that these inmates bring out attention because of their vulnerable health conditions and their high prevalence of health-related risk behaviors. In fact, participants reported some health risk behaviors prior to imprisonment, such as tobacco consumption, drug use, and sexual risk behaviors, but contrary to what other studies 6 have revealed, alcohol abuse before prison was very low, and after imprisonment, it was nearly nonexistent.
Tobacco consumption increased during the women’s imprisonment. Condon et al. 2 stated that the factors brought on by imprisonment conditions, such as increased stress and spare time, along with the availability of the substance itself contribute to this tendency. The consumption of illegal substances, which was significantly high before detention − in accordance with the findings of Staton et al. 16 − was reduced to sporadic occurrences during imprisonment, with no evident signs of addiction. This seems to be related to prisons’ active roles in detoxification from substances. Condon et al. 2 highlighted the fact that most substance users halt their consumption during imprisonment and, although Plugge et al. 17 corroborated this idea, they noted that there is a high percentage of replacement of illegal substances by prescribed medicines such as benzodiazepines and opiates.
Regarding sexual behavior before imprisonment, most of the sexually active participants in this study had had intercourse with only one partner. However, the inconsistent use of condoms combined with the consumption of intravenous substances and prostitution behaviors (even both occur in a lower frequency) increased the possibility of being infected with sexually transmitted diseases.
As expected, during imprisonment, heterosexual activity was significantly reduced, and most inmates had had sexual intercourse with a single partner. However, sexual risk behaviors are still present since condom usage was low. On the other hand, it is worth highlighting that unprotected homosexual intercourse during imprisonment had increased. One possible explanation for the increase in the unprotected homosexual relationships is the unavailability of female condoms in the prison and the low investment in this domain by the health promotion policies. Although studies on sexual risk behavior among female inmates are scarce 6, the revealed behavioral pattern is consistent with what has been observed in the female inmate population, that is, inconsistent condom use, high-risk sexual partners, and prostitution [18 - 20].
Concerning self-harming behaviors, while self-harm during imprisonment was reported by a small number of participants, the prevalence of suicide attempts before and during imprisonment was notable. The percentage of inmates who reported at least one suicide attempt throughout their lifetime was high, emphasizing the female inmate population’s vulnerability to this type of behavior, which has been found in previous studies [ 6 , 21 , 22 ]. This increased vulnerability to the risk of suicide is largely related to the high prevalence of mental illness among the imprisonment population 23, as well as to the high prevalence of adverse experiences. As an example, the results from women inmates’ research indicate that those who have attempted suicide were exposed to more adversity [24, 25]. Considering these data, suicide is a topic that deserves special attention from prison policies in the early identification of female prisoners at risk and the creation of prevention strategies.
Regarding health surveillance before imprisonment, most inmates reported they had seen their GP and/or a health professional in emergency services at least once during the 6 months prior to imprisonment, suggesting that access to community health services is frequent, contrary to what other studies have documented [16, 21, 26 , 27]. However, the reason for this behavior is not included in this study. Future studies should explore the reasons for this active contact with health services prior to imprisonment.
Concerning sexual and reproductive health, menstrual problems were the most relevant issue, which is in line with the findings of a reproductive health study that indicated a higher prevalence of this type of dysfunction among the inmate population in comparison with women in the larger community 28. In contrast, the low percentage of participants who reported having been treated for sexually transmitted diseases seems to indicate, given the tendency toward sexual risk behaviors that was previously noted, a lack of medical care and/or information on this subject 19. Therefore, considering the risk behaviors for both sexually transmitted and chronic diseases (such as uterine cancer) and the lack of medical follow-up and health information, sexual and reproductive health should be an area of attention within prison institutions [29, 30] through the promotion of screening measures and sex education programs.
Moreover, in addition to prisons’ active roles in health education, these institutions are also considered fundamental in the screening and treatment of infectious diseases 31. Following the findings by Barros et al. 31, the prevalence of reported hepatitis C and HIV is prominent. Furthermore, though these diseases have increasingly become the subject of attention of both prison health policies and researchers 21, the high number of inmates with hepatitis C and HIV remains a matter of concern for public health [21, 32 , 33], being the female prison population the most affected [34, 35].
The most frequently reported chronic diseases were migraines, sleeping problems, anxiety, low back pain, and depression, with a notable prominence of mental health complaints and mental disorders, reinforcing, thus, the high prevalence of psychopathology among incarcerated women that has already been reported in numerous studies [7 , 9, 26, 36 , 37].
Still bearing in mind the high number of reported health complaints and illnesses, it is not surprising that there were also a very high percentage of participants in pharmacological therapy. However, it is important to highlight that during the data collection, most participants were unable to specify the substances they were taking, which demonstrates the low inmate knowledge about the medical treatments they were being subjected to. Langner et al. 38 also concluded that there is a higher prevalence of medicine consumption in the female inmate population when compared with the community; in the same way, Butler et al. 5 showed that incarcerated women have a higher percentage of consumption of these substances than their male counterparts. This might happen due to the fact that female detainees have a higher tendency to pursue medical services [27 , 39], which is related to the previously mentioned high rates of diseases and health complaints, as well as the replacement of illegal drugs by psychotropic medication.
Theeported health complaints were frequent, which corroborates the findings of Butler et al. 5 and Robert et al. 27, indicating that health complaints among female inmates are frequent during imprisonment. This might be a result not only of their vulnerability in terms of mental and physical health, but also of the increase in self-awareness due to their imprisonment 27. The high prevalence of anxiety-related complaints is a sign of psychological stress among female inmates.
Finally, considering the participants’ general health, it is possible to conclude that they have lower levels of physical and mental health compared with the community female population, which is similar to the findings of Plugge and Fitzpatrick 9 in the United Kingdom and of Butler et al. 5 in Australia. In addition, it is not surprising that more than half of the participants in this study reported negative perceptions of their health not only because of the pattern of health risk behaviors, but also due to the prevalence of infectious and mental diseases, the high consumption of prescribed drugs, and the plethora of health complaints.
However, we need to note some findings that could be related to a positive impact of prison on participant health, such as the above-mentioned decrease in the consumption of illegal substances and alcohol. These facts could contribute to the high percentage of women who reported health status improvement during imprisonment. In contrast, some findings could be related to the negative impact of prison on participants’ health, such as the already mentioned increase in smoking and the psychological stress related to imprisonment, which can explain the percentage of women who evaluate their health as worse or much worse. These results reveal how prison impact can be variable 2.
This study had some limitations, of which the most important was the number of participants, which represented only 31.1% of the imprisoned females in Portugal in the first quarter of 2012. Nevertheless, the sociodemographic and juridical characteristics of the studied sample are similar to the most common among the overall Portuguese female inmate population at the time of the data collection. Another limitation concerns the questionnaire on risk behavior and health records that had no consistent timeline that determines when the issues addressed had occurred, making it more difficult to thoroughly analyze these participants’ risk behaviors and health histories before and during imprisonment. The fact that this study is based on self-reporting is most likely its greatest limitation, due to the implied bias associated with this type of measure. Even so, there are no signs that inmates are less trustworthy than the overall population, and self-reporting instruments such as the SF-12 are valid when applied to the incarcerated population [9, 17]. Giving the relevance of obtaining health outcomes through other sources of information rather than self-report, an a posteriori study was carried out on the female prisoners’ health in Portugal on the basis of information contained in the clinical trials [Alves and Costa Maia, in press].
Our results emphasized the vulnerable health status of detained women and the variable impact of imprisonment on health. These seemingly fragile health conditions of the women continue to draw attention to the need for politicians, prison management, health advocates, and prison staff to invest in programs and measures focused on improvements in female inmates’ health. Bergh et al. 40 mentioned the need to change criminal justice systems, considering the failures in gender sensitivity. They highlight 4 crucial steps for action that we would also like to underline since they synthesize some of the most important changes, considered in the literature, for health improvements of women prisoners: imprisonment of women should be considered only when all other alternatives are unavailable or unsuitable; all staff working with women prisoners should have followed gender sensitivity training to raise awareness of and improve response to these gender-related issues; the European Prison Rules are of vital importance, but they need a revision to guarantee the provision of services to meet women prisoners’ specific needs; health services for women in prison should be individualized as far as possible to meet their specific expressed needs. These efforts will promote improvement not only in these women’s lives but also those of their communities because their reentries will potentially be more successful. Finally, our findings should encourage future research using qualitative methods in order to better understand how they perceive their health and which factors are involved in the emotional and physical changes that affect these perceptions.
1 Wolff H, Sebo P, Haller DM, Eytan A, Niveau G, Bertrand D, et al: Health problems among detainees in Switzerland: a study using the ICPC-2 classification. BMC Public Health 2011; 11: 245. 10.1186/1471-2458-11-245 21504562 [ Links ]
2 Condon L, Hek G, Harris F: A review of prison health and its implications for primary care nursing in England and Wales: the research evidence. J Clin Nurs 2007; 16: 1201–1210. 10.1111/j.1365-2702.2007.01799.x 17584337
3 Lindquist CH, Lindquist CA: Health behind bars: utilization and evaluation of medical care among jail inmates. J Community Health 1999; 24: 285–303. 10.1023/A:1018794305843 10463472
4 Freudenberg N, Moseley J, Labriola M, Daniels J, Murrill C: Comparison of health and social characteristics of people leaving New York City jails by age, gender, and race/ethnicity: implications for public health interventions. Public Health Rep 2007; 122: 733–743. 10.1177/003335490712200605 18051666
5 Butler T, Kariminia A, Levy M, Murphy M: The self-reported health status of prisoners in New South Wales. Aust NZ J Public Health 2004; 28: 344–350. 10.1111/j.1467-842X.2004.tb00442.x 15704699
6 Harris F, Hek G, Condon L: Health needs of prisoners in England and Wales: the implications for prison healthcare of gender, age and ethnicity. Health Soc Care Community 2007; 15: 56–66. 10.1111/j.1365-2524.2006.00662.x 17212626
7 Plugge E, Douglas N, Fitzpatrick R: Patients, prisoners, or people? Women prisoners’ experiences of primary care in prison: a qualitative study. Br J Gen Pract 2008; 58: 630–636. 10.3399/bjgp08X330771 18801272
8 Harner HM, Riley S: Factors contributing to poor physical health in incarcerated women. J Health Care Poor Underserved 2013; 24: 788–801. 10.1353/hpu.2013.0059 23728045
9 Plugge E, Fitzpatrick R: Assessing the health of women in prison: a study from the United Kingdom. Health Care Women Int 2005; 26: 62–68. 10.1080/07399330590885768 15764461
10 Binswanger I, Krueger PM, Steiner JF: Prevalence of chronic medical conditions among jail and prison inmates in the USA compared with the general population. J Epidemiol Community Health 2009; 63: 912–919. 10.1136/jech.2009.090662 19648129
11 Moschetti K, Stadelmann P, Wangmo T, Holly A, Bodenmann P, Wasserfallen JB, et al: Disease profiles of detainees in the Canton of Vaud in Switzerland: gender and age differences in substance abuse, mental health and chronic health conditions. BMC Public Health 2015; 15: 872. 10.1186/s12889-015-2211-6 26358116 [ Links ]
12 Haes J, Van Knippenberg F, Neijt J: Measuring psychological and physical distress in cancer patients: structure and application of Rotterdam Symptom Checklist. Br J Cancer 1990; 62: 1034–1038. 2257209
13 Maia A, McIntyre T, Pereira MG, Ribeiro E: War exposure and post-traumatic stress as predictors of Portuguese colonial war veterans’ physical health. Anxiety Stress Coping 2011; 24: 309–325. 10.1080/10615806.2010.521238 20945238
14 Ware JE, Kosinski M, Keller SD: A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care 1996; 34: 220–233. 10.1097/00005650-199603000-00003 8628042
15 Pais-Ribeiro J: O importante é a saúde: estudo de adaptação de uma técnica de avaliação do estado de saúde-SF-36. Lisboa, Fundação Merck Sharp & Dohme, 2005. [ Links ]
16 Staton M, Leukefeld C, Webster JM: Substance use, health, and mental health: problems and service utilization among incarcerated women. Int J Offender Ther Comp Criminol 2003; 47: 224–239. 10.1177/0306624X03251120 12710367
17 Plugge E, Yudkin P, Douglas N: Changes in women’s use of illicit drugs following imprisonment. Addiction 2009; 104: 215–222. 10.1111/j.1360-0443.2008.02419.x 19149815
18 Clarke JG, Hebert MR, Rosengard C, Rose JS, Silva KM, Stein MD: Reproductive health care and family planning needs among incarcerated women. Am J Public Health 2006; 96: 834–839. 10.2105/AJPH.2004.060236 16571701
19 Miranda A, Merçon-de-Vargas P, Viana M: Saúde sexual e reprodutiva em penitenciária feminina, Espírito Santo, Brasil. Rev Saúde Pública 2004; 38: 255–260.
20 Sufrin CB, Tulsky JP, Goldenson J, Winter KS, Cohan DL: Emergency contraception for newly arrested women: evidence for an unrecognized public health opportunity. J Urban Health 2010; 87: 244–253. 10.1007/s11524-009-9418-8 20012702
21 Fazel, S, Baillargeon J: The health of prisoners. Lancet 2011; 377: 956–965. 10.1016/S0140-6736(10)61053-7 21093904
22 Ginn S, Robinson R: Women prisoners. BMJ 2013; 8318: 1–4.
23 Baillargeon J, Penn JV, Thomas CR, Temple JR, Baillargeon G, Murray OJ: Psychiatric disorders and suicide in the nation’s largest state prison system. J Am Acad Psychiatry Law 2009; 37: 188–193. 19535556
24 Alves J, Maia A: Experiências adversas durante a infância e comportamentos de risco para a saúde em mulheres reclusas. Psic Saúde Doenças 2010; 11: 151–171.
25 Marzano L, Hawton K, Rivlin A, Fazel S: Psychosocial influences on prisoner suicide: a case-control study of near-lethal self-harm in women prisoners. Soc Sci Med 2011; 72: 874–883. 10.1016/j.socscimed.2010.12.028 21345561
26 Baillargeon J, Black SA, Pulvino J, Dunn K: The disease profile of Texas prison inmates. Ann Epidemiol 2000; 10: 74–80. 10.1016/S1047-2797(99)00033-2 10691060
27 Robert D, Frigon S, Belzile R: Women, the embodiment of health and carceral space. Int J Prisoner Health 2007; 3: 176–188. 10.1080/17449200701520099
28 Allsworth JE, Clarke J, Peipert JF, Hebert MR, Cooper A, Boardman L: The influence of stress on the menstrual cycle among newly incarcerated women. Women Health Issues 2007; 17: 202–209. 10.1016/j.whi.2007.02.002 17560123
29 Binswanger I, White MC, Pérez-Stable EJ, Goldenson J, Tulsky JP: Cancer screening among jail inmates: frequency, knowledge, and willingness. Am J Public Health 2005; 95: 1781–1787. 10.2105/AJPH.2004.052498 16186455
30 Sufrin CB, Creinin MD, Chang JC: Contraception services for incarcerated women: a national survey of correctional health providers. Contraception 2009; 80: 561–565. 10.1016/j.contraception.2009.05.126 19913150
31 Barros H, Ramos E, Lucas R: A survey of HIV and HCV among female prison inmates in Portugal. Cent Eur J Public Health 2008; 16: 116–120. 18935775
32 Thein H, Butler T, Krahn M, Rawlinson W, Levy MH, Kaldor JM, et al: The effect of hepatitis C virus infection on health-related quality of life in prisoners. J Urban Health 2006; 83: 275–288. 10.1007/s11524-005-9015-4 16736376
33 Torres A, Gomes M: Drogas e prisões: relações próximas. Toxicodependências 2005; 11: 23–40.
34 Altice FL, Marinovich A, Khoshnood K, Blankenship KM, Springer S, Selwyn P: Correlates of HIV infection among incarcerated women: implications for improving detection of HIV infection. J Urban Health 2005; 82: 312–326. 10.1093/jurban/jti055 15872190
35 Nijhawan AE, Salloway R, Nunn AS, Poshkus M, Clarke JG: Preventive healthcare for underserved women: results of a prison survey. J Women Health 2010; 19: 17–22. 10.1089/jwh.2009.1469 20088654
36 Alves J, Dutra A, Maia Â: História de adversidade, saúde e psicopatologia em reclusos: comparação entre homens e mulheres. Cienc Saúde Coletiva 2013; 18: 701–710.
37 Moloney KP, Moller LF: Good practice for mental health programming for women in prison: reframing the parameters. Public Health 2009; 123: 431–433. 10.1016/j.puhe.2009.04.007 19482320
38 Langner N, Barton J, McDonagh D, Noel C, Bouchard F: Rates of prescribed medication use by women in prison. Forum Correct Res 2002; 14: 10–14.
39 Feron JM, Paulus D, Tonglet R, Lorant V, Pestiaux D: Substantial use of primary health care by prisoners: epidemiological description and possible explanations. J Epidemiol Community Health 2005; 59: 651–655. 10.1136/jech.2004.022269 16020641
40 Bergh BJ, Gatherer A, Fraser A, Moller L: Imprisonment and women’s health: concerns about gender sensitivity, human rights and public health. Bull World Health Organ 2011; 89: 689–694. 10.2471/BLT.10.082842 21897490
Received: December 7, 2016
Accepted: May 22, 2017

