











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Alcohol consumption is a significant risk factor contributing to the global burden of mortality and disabilities 1. According to the World Health Organization (WHO), harmful alcohol consumption was responsible for 3 million deaths (accounting for 5.3% of all deaths) and 132.6 million disability-adjusted life years (DALYs) in 2016, corresponding to 5.1% of all DALYs 2. Notably, the mortality associated with alcohol consumption surpasses that caused by diseases such as tuberculosis, HIV/AIDS, and diabetes. Specifically, in 2016, alcohol consumption led to 2.3 million deaths and 106.5 million DALYs among men, while women experienced 0.7 million deaths and 26.1 million DALYs attributable to alcohol consumption. Geographically, the burden of disease and injury attributable to alcohol consumption, when age-standardized, exhibits regional variations across WHO regions 2.
In 2018, the prevalence of current alcohol use among young adults aged 18-25 years was 55.1%, corresponding to approximately 18.8 million individuals 3. Furthermore, studies have indicated that mortality rates attributed to alcohol tend to be higher among middle-aged and older adults, whereas the burden of alcohol-related disabilities is often concentrated among younger individuals 4. Globally, men exhibit a higher frequency of alcohol consumption compared to women 2. However, it is important to note that the prevalence of alcohol consumption varies based on cultural norms and standards within different countries. For example, Nordic countries and Eastern European countries, in general, tend to have higher rates of alcohol consumption in comparison with Southern European countries 5.
Understanding global trends in population health and changes in the primary sources of disease burden over time is essential for monitoring progress toward the Sustainable Development Goal of ensuring healthy lives and well-being. To achieve a robust assessment of these trends, the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) provides the latest epidemiological data, assisting countries in identifying priorities and challenges in their pursuit of the goal across various age and sex groups in 204 countries and territories 6.
This study aimed to analyze the GBD results for alcohol use disorder (AUD) in Estonia from 1990 to 2019. Specifically, we will investigate the incidence, prevalence, mortality, years of life lost (YLL), years living with disabilities (YLDs), and DALYs associated with AUD. By examining these variables, our study seeks to identify new trends and progress related to AUD in Estonia over the specified period. Additionally, we will explore any potential disparities or specific considerations related to childhood sexual abuse (CSA) and its implications for AUD. CSA is a recognized risk factor for alcohol-related problems in both adolescence and adulthood, with a potentially stronger impact on women. Research has shown that CSA is linked to increased heavy drinking among adult women, particularly when combined with physical abuse. Moreover, childhood maltreatment, including sexual abuse, predicts alcohol abuse or dependence during adolescence, which then contributes to excessive drinking in adulthood, especially among women 7. By drawing implications from our findings, we aim to contribute to future research endeavors and provide valuable insights for policymakers, aiding their understanding of the current challenges in the field of public health.
Material and Methods
Population and Sample
In our study, we focus on the population of Estonia from 1990 to 2019. The GBD study, which serves as the primary data source for our analysis, provides comprehensive epidemiological data for 204 countries and territories. The GBD study covers various age groups and both sexes, allowing for a comprehensive assessment of AUD incidence, mortality, and DALYs across different population segments. However, it is important to note that our study does not involve a specific sample as it relies on aggregated population-level data from the GBD study 8.
Data Accessibility
The GBD study data are accessible through the Institute for Health Metrics and Evaluation (IHME) website (http://www.healthdata.org/gbd). The IHME provides access to a wide range of GBD estimates, including mortality, DALYs, incidence, and prevalence rates for numerous health conditions and risk factors. Detailed information on data availability, methodology, and specific variables can be obtained from the IHME website, which serves as the official repository for GBD study data.
Definitions
In epidemiology, several key indicators are used to evaluate the occurrence and impact of specific conditions within populations. Incidence refers to the rate at which new cases of a particular condition emerge over a specified period, reflecting the occurrence rate of new instances. Prevalence, on the other hand, represents the overall number of individuals affected by a specific condition within a designated timeframe or at a given point in time, serving as a measure of the proportion or percentage of affected individuals in the population. Mortality encompasses the number of deaths attributed to a specific condition within a predetermined period, providing insights into the associated death rate. YLL is a concept that quantifies the impact of premature death by estimating the number of potential YLL due to a specific condition, considering the discrepancy between the age at death and a standard life expectancy. YLD is a metric used to evaluate the burden of living with a specific condition by estimating the number of years individuals spend with a disability. It considers the condition's impact on an individual's quality of life, productivity, and overall well-being. DALYs represent a comprehensive measure of the overall disease burden, as they combine the YLL and the YLD. DALYs provide an assessment of the total number of healthy years lost due to a specific condition, taking into consideration both premature mortality and disability 9.
Statistical Analysis
In this study, descriptive statistics were presented using age-standardized rates or percentages along with corresponding 95% confidence intervals, as provided by the GBD study. To assess the trends of various indices, including DALY, incidence, mortality, and 1-mortality-to-incidence ratio (1-MIR), joinpoint regression analysis was employed. These indices served as inputs for the joinpoint regression model, enabling the estimation of annual percent change (APC) between two consecutive trend-change points as follows 10:
 ***
***
where x is the year and coefficients (b0 and b1) are the parameter estimates. In addition, the average APC (AAPC) was calculated as the average mean of the estimated percent changes over the study period. If no significant trends were observed, the APC and AAPC values were equal. However, if significant trends were detected, different APCs were estimated for each direction. To assess the statistical significance of the estimation, the 95% confidence interval of the APC was also computed. The permutation test was used to obtain the number of joinpoints of each index during the study period. The permutation test was employed to determine the number of joinpoints for each index during the study period. This was accomplished using the Joinpoint Regression Program, Version 4.9.0.0 (Statistical Research and Applications Branch, National Cancer Institute) 11,12. To test for parallelism between sexes, Kmax joinpoints were considered, where Kmax is greater than or equal to the number of joinpoints for both groups under the null hypothesis of parallelism and alternative hypothesis of lack of parallelism 13.
Results
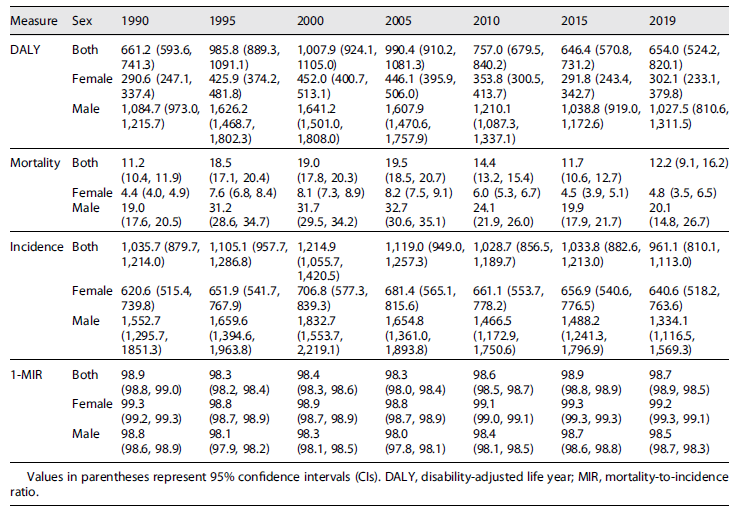
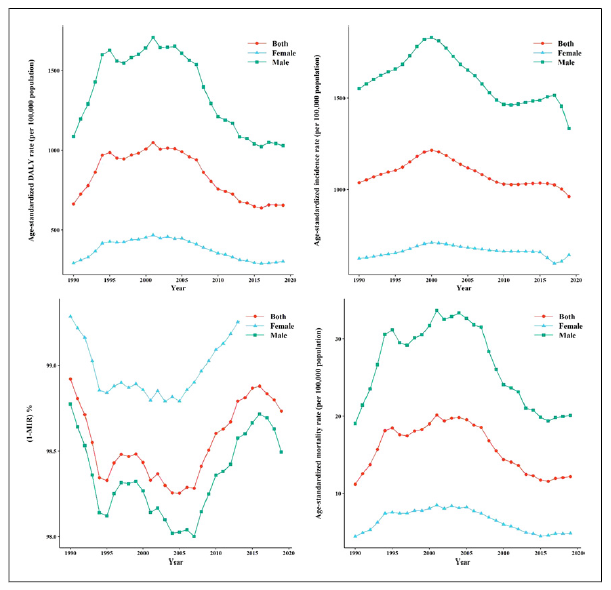
This study presents an analysis of Estonia’s DALYs, mortality, incidence, and 1-MIR related to AUDs from 1990 to 2019. Descriptive statistics for these indices are provided in Table 1, stratified by gender and years (1990, 1995, 2000, 2005, 2010, 2015, and 2019). The trends of these indices over the years are visualized in Figure 1. The DALY, incidence, and mortality exhibited upward and downward trends from 1990 to around 2000 and 2000 to 2019, respectively. In contrast, the 1-MIR index demonstrated a reverse trend compared to the previous indices. Furthermore, all indices were consistently higher in males compared to females throughout the study period.
Table 1 Descriptive statistics for age-standardized rates (including DALY, mortality, incidence per 100,000) and 1-MIR (%) of AUD by gender from 1990 to 2019
Next, joinpoint regression models were fitted to the age-standardized rates of DALY, mortality, incidence, and 1-MIR, as shown in Table 2. For total DALY rates, the AAPC was zero, indicating no significant change in AAPC over the study period. However, three joinpoints were identified in 1994, 2004, and 2014, resulting in four distinct periods and trends. The APCs were 9.6, 0.8, −4.5, and 0.1 for the time intervals 1990-1994, 1994-2004, 2004-2014, and 2014-2019, respectively. The first three APCs were significant, with the highest increase observed in the first trend (1990-1994) and the highest reduction in the third interval (2004-2014). Similar trends were observed in total mortality rates using the fitted joinpoint regression. Three joinpoints were observed in 1994, 2005, and 2015, leading to four distinct periods and trends. The APCs were 12.3, 1.1, −5.4, and 1.8 for the time intervals 1990-1994, 1994-2005, 2005-2015, and 2015-2019, respectively. The highest increase and reduction occurred, respectively, in the first time interval (1990-1994) and the third one (2005-2015). The AAPC of total incidence showed a very slight reduction with a value of −0.3. Four joinpoints were identified in 1996, 2000, 2010, and 2017, resulting in five distinct periods and trends. The second trend (1996-2000) showed the highest increase in APC, while the highest reduction was reported in the last trend (2017-2019). Regarding the total 1-MIR index, the AAPC was zero and nonsignificant. However, five joinpoints were estimated in 1994, 1998, 2005, and 2015, leading to five distinct periods and trends. The maximum reduction in APC was observed in the first period (1990-1994), with an APC of −0.2. The highest increase was seen in the fourth period (1998-2005), with an APC of 0.1. Figure 2 compares the behavior of these four indices over the study period among men, women, and both genders using the fitted joinpoint regression. The results demonstrate slightly different trends of the indices between men and women.
Table 2 Results of the joinpoint regression analysis of DALY, mortality, incidence, and 1-MIR of AUD in Estonia population from 1990 to 2019
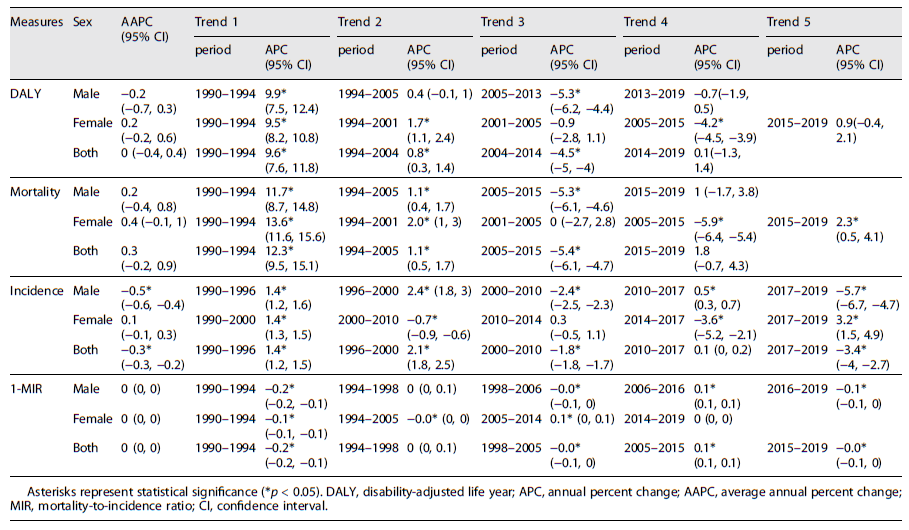
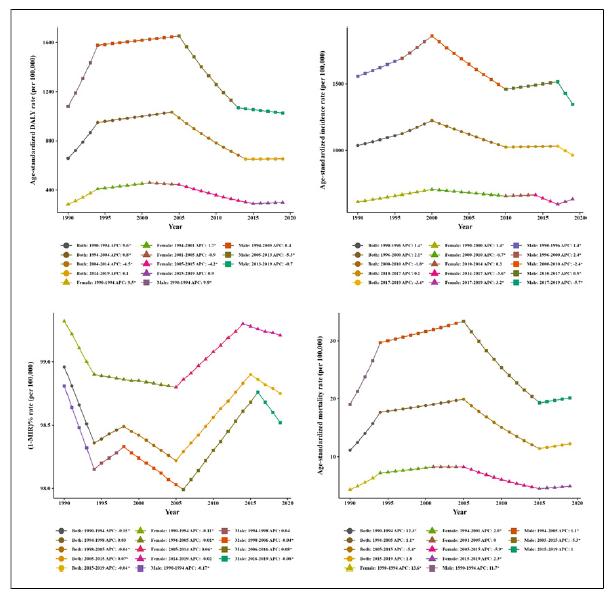
Fig. 2 Results of joinpoint regression analysis of DALY, mortality, incidence, and 1-MIR in Estonia population from 1990 to 2019.
APC values were reported for age-standardized mortality rates and DALY rates (per 100,000) by sex among victims of CSA. For total cases, females, and males, three, four, and three joinpoints were identified, respectively, indicating different trends in DALY and age-standardized mortality rates. Table 3 presents the nonparallel trends of age-standardized mortality rates between females and males (p value <0.001), as well as in total cases (p value <0.001). Similarly, there was a lack of parallelism in the trend of DALY rates between both females (p value <0.001), both males (p value = 0.002), and female-male (p value <0.001) Figure 3.
Table 3 The comparison of Parallelism in age-standardized DALY and mortality rate (per 100,000) among those with CSA by sex
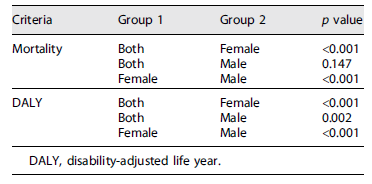
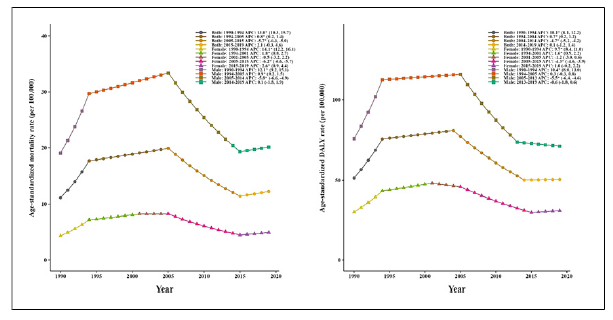
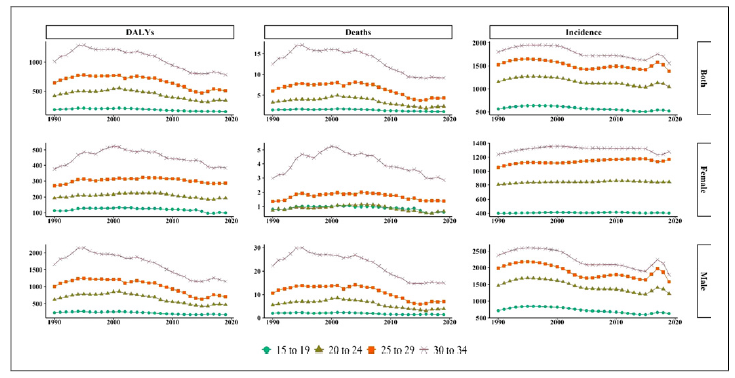
Figure 4 illustrates the changing trends in DALYs, deaths, and incidence rates due to AUDs by age group for each gender over the past 30 years in Estonia. Among female subjects, the incidence rates for all age groups remained relatively stable from 1990 to 2019. Similar trends were observed for deaths and DALYs across different age groups among female patients throughout the study period, with almost constant changes per age group. Consistent with the changes in DALYs, deaths, and incidence rates in both sexes, the rates showed a slow decline in each age group among males.
Discussion
The present study aimed to assess the temporal trends of DALY, mortality rate, incidence rate, and the 1-MIR of AUD in Estonia from 1990 to 2019. The findings revealed an overall declining trend in the incidence rate of AUD over the study period. Conversely, the average DALY, mortality, and 1-MIR trends remained relatively stable and did not exhibit significant variations throughout the study period. Notably, three change points were identified in DALY and mortality, while four change points were observed in incidence and 1-MIR of AUDs. The initial trends for DALYs, mortality, and incidence demonstrated an upward trajectory, followed by a subsequent significant decline. Furthermore, a slight yet significant change in 1-MIR was noted. These trends exhibited a pattern of initial decrease, subsequent increase, and subsequent decrease once more. It is worth mentioning that the rates of MIR, DALY, mortality, and incidence were consistently higher among men compared to women. However, it is important to note that the trends in these indicators exhibited parallel changes for both men and women.
The current study showed a higher decrease in the incidence of AUDs among men compared with women from 1990 to 2019. The incidence of AUDs significantly increased from 1990 to 2000, then decreased from 2010 to 2018, and continued to decline from 2017 to 2019. In a study conducted by Vuik and Cheatley, similar results were found. Although the incidence of alcohol consumption decreased in Estonia between 2010 and 2018, the decline in alcohol consumption was higher among men 14. Additionally, consistent results were also seen in WHO studies in Estonia between 1992 and 1999. In this regard, the consumption of pure alcohol by adults (15 and older) increased from 7.8 to 8.8 L per year 15. Cultural factors and social undesirability can be attributed to the lower level of alcohol consumption in women 16. Consistent results also had been presented by McKee et al. 17 that alcohol consumption is a threat to public health in Baltic countries, while almost one in 10 Estonian men drink 80 g per day. This quantity of drinking alcohol correlates with a considerably enhanced danger of various physical problems. By our findings, hence alcohol consumption is attributed to physical harm and death, whether directly or indirectly, premature death in men makes up to 70 percent of all deaths, and alcohol is a cause of death 18, and in Estonia, the rate of mortality among men was dramatically higher than women 19. However, the number of premature death caused by alcohol since 2010 has been decreasing 18. This finding parallels Janssen et al. 20, referring that Eastern European countries are experiencing high levels of alcohol-attributable mortality, significantly among men, with growths specifically in the 1990s, followed by recent declines.
Our results provide insights into the trends and patterns of CSA victims in Estonia. The study examined various indices, including DALY, mortality, incidence, and 1-MIR, over the period from 1990 to 2019. The findings revealed different periods and trends, indicating significant changes in the rates over time. When focusing specifically on CSA victims, gender differences were observed, with the trend of DALY and age-standardized mortality rates differing significantly between females and males, as well as overall cases. The results indicated that females who experienced CSA were particularly vulnerable to adult binge drinking, suggesting long-lasting effects beyond the initial abuse. These effects were not limited to the adolescent period and may be related to self-harm behaviors observed in sexually abused women. However, the relationship with adult binge drinking was not as evident for males who experienced other forms of abuse, such as physical or emotional abuse or neglect. Furthermore, family alcohol problems had different effects on adolescent drinking and norms for males and females 21-23. While these findings provide important insights into the impact of CSA on adult binge drinking, further research is needed to explore the underlying mechanisms and potential protective factors. It is essential to develop tailored interventions that consider the persistent consequences of CSA and include prevention components for alcohol and binge drinking among women who have experienced sexual abuse. However, these findings must be interpreted in light of alcohol policies in Estonia. In 1985, an anti-alcohol campaign established massive propaganda and raised the price of alcoholic beverages; despite substantial results, the campaign collapsed. This restriction dramatically increased the number of illegal alcohol production markets, and the campaign was not popular among consumers 24.
Moreover, reestablishing Estonia’s independence in 1991 had numerous impacts on different aspects of life and caused profound changes, including the alcohol market. The assortment, production, and quantities of alcohol increased explosively. The distribution policies of alcohol made it more accessible to society; particularly between 1993 and 1995, the number of alcohol selling points soared to 80 percent 24.
Between 2000 and 2017, a transformation happened in Estonia’s type of alcoholic beverages that directed to a considerable reduction in strong and light alcoholic beverage consumption. This transition from health-related issues was meaningful 25. This study explains our findings and the decreasing trend in alcohol consumption in the context of economic stabilization and the more restricted implementation of health policies from the mid-2000s 26. These changes in alcohol consumption trends came along with rules on production and sale and increased alcohol taxes in the Baltic countries 20.
This study possesses both strengths and limitations, similar to other research endeavors. A significant strength lies in its longitudinal design, which allows for examining alcohol-related problems over an extended period and facilitates predictions regarding future trends. Additionally, using data from the GBD study ensures the utilization of high-quality information regarding alcohol consumption. The availability of government policies and tax records enables the extraction of reliable data on recorded alcohol consumption. However, it is essential to acknowledge that uncertainties exist regarding unrecorded consumption, including alcohol produced illegally or through homemade methods. While this research focused on analyzing trends and alcohol-related issues among individuals aged 15 to 34 in both genders, it should be noted that the available data need to adequately capture the younger population and the early onset of alcohol drinking.
Further research targeting youth drinking behavior would be valuable in predicting initial alcohol consumption patterns among the next generation. Despite the novelty of studying trends in Estonia based on GBD data from 1990 to 2019, additional research still needs to be conducted. Future investigations can explore additional variables related to alcohol-related issues, providing a more comprehensive understanding of the topic. Furthermore, conducting comparative studies across countries with varying socioeconomic factors would shed further light on this complex issue.
Conclusion
The present study provides a longitudinal assessment of trends in AUD in Estonia, offering insights into the changing patterns of alcohol consumption across genders. Our findings reveal higher rates of the MIR, DALY, mortality, and incidence of AUDs among men compared to women. However, the observed pattern is not linear, indicating the need for future investment in the implementation of new policies and prevention programs targeting alcohol-related mortality and alcohol consumption, particularly among older age groups.
The novelty of our methodology allowed us to obtain a realistic estimation of alcohol-related issues across genders and age groups, offering valuable insights into past trends in Estonia. Nonetheless, it is important to note that the decline observed in these trends does not necessarily imply that excessive alcohol consumption has been effectively controlled. Continued efforts are required to address this ongoing public health concern.
Statement of Ethics
Due to using the IHME database, ethical approval and consent were not required as this study was based on publicly available data. We have utilized the Global Burden of Disease Study database and have cited it according to the proposed format of the Institute for Health Metrics and Evaluation.
Funding Sources
The current research acquired no specific Grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Contributions
F.Z. conceived the study. M.A.L. extracted the data, reworked them for analysis, and conducted the analysis. F.Z. and M.A.L. interpreted the results and drafted the manuscript and the supplementary document. All authors have read and agreed to the published version of the manuscript.
Data Availability Statement
We confirm that all methods were performed by the relevant guidelines and regulations. The datasets analyzed during the current study are available in GBD database: http://ghdx.healthdata.org/gbd-results-tool.

