











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Titanium has been considered to be a nonallergenic material, so it has been used in orthopaedic and spinal surgery, pacemakers, clips, coils and dental implants. Recent studies have reported rare cases of metal allergy caused by titanium-containing materials.
There are no standardized diagnostic tests and titanium allergy is often a diagnosis of exclusion.
We present a rare case of a confirmed metal allergy to a titanium plating system.
Case report
We describe the case of a 53-year-old male patient with priors of psoriasis, controlled with topical therapy. He had no history of atopy or contact reactions to metals.
The patient suffered a left tibial plateau fracture after a fall and underwent orthopedic surgery for open reduction and internal fixation with a titanium plating system. There were no complications during surgery or in the immediate postoperatory period. The patient was discharged, with indications to complete a physiotherapy treatment plan which he began right away and completed after a few months, with regained mobility and muscle strength.
Almost 1 year later, the patient was referred to the dermatology department as he continued to complain of chronic pain and edema at the site of the implant on the left leg with two subcutaneous nodules that had developed 3 months after the surgery.
On dermatological examination, the patient had a linear surgical scar on the left leg without erythema or induration but with tenderness to touch and two fluctuating soft and elastic subcutaneous skin-colored nodules beneath the distal part of the scar. These nodules were mobile with the movements of the leg muscles (Fig. 1). There was no evidence of infection, loosening or failure of the metal plate.

Figure 1 Well-healed linear surgical incision on the left leg with two fluctuating subcutaneous nodular lesions beneath the distal part of the incision.
In order to exclude a hypersensitivity reaction, patch testing was performed with the baseline series and an extended metal series (Chemotechnique diagnostics, Vellinge, Sweden). Readings were performed on the day (D) 3 and D7, according to European Society of Contact Dermatitis guidelines.
On D3, there were positive reactions to nickel sulfate 5% pet (++), titanium (IV) oxalate hydrate 5% pet (++), sodium tetrachloropalladate (II) hydrate 3% pet (+) and rhodium (III) chloride hydrate 2% pet (++). At D7 persisted the positive reactions to nickel sulfate 5% pet (++), titanium (IV) oxalate hydrate 5% pet (++) and sodium tetrachloropalladate (II) hydrate 3% pet (+), supporting the hypothesis of titanium hypersensitivity secondary to the recent implantation (Fig. 2-3).
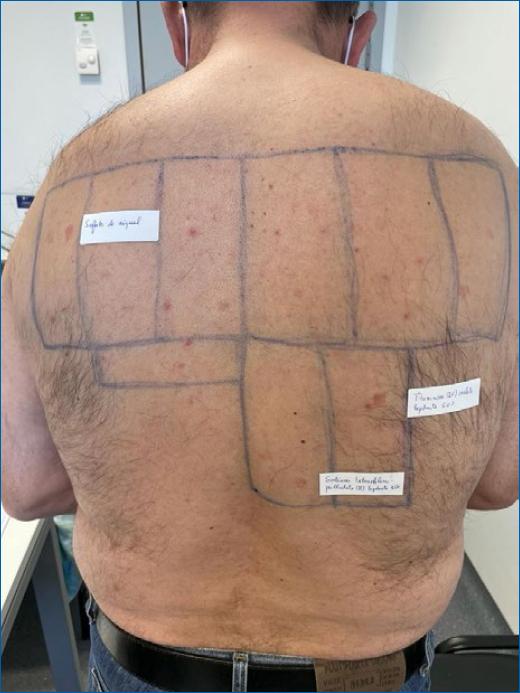
Figure 2 Result of patch testing at D7-allergy-positive reaction to nickel sulfate, titanium (IV) oxalate hydrate 5% and sodium tetrachloropalladate (II) hydrate.

Figure 3 Result of patch testing at D7-allergy-positive reaction to titanium (IV) oxalate hydrate 5% and sodium tetrachloropalladate (II) hydrate.
The patient underwent removal of the titanium plating system on the left leg and 1 month after surgery, there was complete healing with no inflammatory signs, no pain or functional limitations, and the nodular lesions are no longer perceptible.
Discussion
Titanium is considered the most biocompatible metal due to its corrosion resistance, bio-inertness, osseointegration capacity and high fatigue limit. Therefore, it is widely used in the medical field, such as plastic surgery, dental implants, pacemakers, neurosurgery and orthopedic surgery, significantly increasing exposure to this rare metal1,2.
Despite its known biocompatibility, several studies have reported cases of suspected and confirmed allergic reactions to titanium salts, including two Portuguese case reports3-12. Most are related to dental implant prostheses and screw fixation systems. One case occurred in a patient with allergic contact dermatitis who had dental implant prostheses and who exhibited allergic symptoms after orthopedic surgery2.
In our case, the patient had no priors of atopy or contact reactions to metals and developed the symptoms after an orthopaedic surgery with the implantation of a titanium plating system.
Allergic reactions to titanium described in the literature are varied and include rash, urticaria, pruritus, oedema, eczematous lesions, hyperplastic lesions of soft tissue, impaired healing fractures, pain, and necrosis around the implants9. However, most instances of titanium allergy appear as dermatitis around titanium products and symptoms resolve after the removal of the offending agent13.
In this case, the patient displayed pain, oedema and subcutaneous lesions on the site of the titanium implant, which raised the suspicion of titanium allergy.
Diagnosing titanium allergy is complicated because of the low sensitivity and specificity of the diagnostic tests available. The skin patch test has not yet been developed as the valid standardized test for titanium allergy and positive reactions to titanium have only rarely been demonstrated with skin testing14. The most widely used patch test preparation is titanium dioxide, but some studies suggest using other titanium salts as alternative reagents, such as 0.1 and 0.2% titanium sulfate in water solution or 0.1 and 0.2% titanium chloride pet15, 0.1% titanium tetrachloride2 or titanium oxalate hydrate 5% pet, but it is yet to be confirmed which is the most adequate.
In this case, we used titanium oxalate hydrate 5% pet and obtained a positive test reaction at D3 that persisted at D7, ruling out irritation.
Before surgical implants, patients should be asked about a history of reactions to metals and patch testing should be recommended for those who have experienced such reactions.

