{kind=link}
{kind=link}
The cost effectiveness of a low clearance nephrology care
O custo-benefício de uma consulta de baixa depuração
Anabela Malho Guedes1,2,3, Ana Paula Silva1,2,3, Carlos Goncalves4, Sandra Sampaio1, Elsa Morgado2, Patricia Mendes3, Isilda Bexiga3, Viriato Santos1, Idalecio Bernardo1, Pedro Leao Neves1,2,3
1Department of Nephrology, Centro Hospitalar do Algarve. Faro, Portugal
2Department of Biomedical Sciences, Universidade do Algarve.Faro, Portugal
3Nephrocare. Faro, Portugal
4Nephrocare. Lisboa, Portugal
]]>
ABSTRACT
Background: The projected growth in spending for the treatment of end-stage renal failure threatens to become unsustainable for most countries. Different sources suggest that patients with progressive chronic kidney disease should be managed in a multidisciplinary care setting. Given that multidisciplinary teams impact on health care resources, it is imperative to evaluate their effectiveness. The purpose of this study was to evaluate the impact of exposure to conventional nephrology care or low clearance nephrology care (LCC) prior to dialysis initiation on patient outcomes and expenditure after dialysis initiation. Methods: This study considered incident haemodialysis patients attending the LCC vs. receiving standard nephrologist care at our Centre, between 2008 and 2011. Costs were calculated based on the Portuguese capitation system introduced in 2008. Results: During the evaluation period, 176 patients initiated dialysis, 113 exposed to the LCC and 63 received standard nephrologist care. There were no demographic differences between groups. The LCC group started dialysis with higher eGFR (10.1 vs. 8.3 ml/min/1.73m2, p = 0.002), higher albumin (3.8 vs. 3.5 g/dl, p = 0.020), lower PTH (549.7 vs. 841.1 pg/ml, p = 0.008); in this group, a higher proportion of patients started dialysis with a definitive vascular access (85.8% vs. 65.5%, p = 0.002). The biochemical parameters were comparable after 6 and 12 months, but the costs to achieve the same analytical objective were much lower in the LCC group: 3737.7 vs. 5087.3 euros (p = 0.005) and 6336.4 vs. 8024.6 euros (p = 0.035) after 6 and 12 months, respectively. There were no differences in survival or morbidity between groups. Older age was associated with greater risk of hospitalization (p = 0.032) and death (p < 0.001); a definitive vascular access correlated with lower hospitalization (p = 0.006) and a trend to lower risk of death (p = 0.051). Conclusions: Better biochemical variables and presence of a definitive vascular access at dialysis initiation in the LCC, resulted in a lower expenditure during the first year of haemodialysis.
Key-Words: Chronic kidney disease; cost effectiveness; low clearance clinic; multidisciplinary team; predialysis care.
RESUMO
O crescimento projectado do custo do tratamento da doença renal crónica avançada ameaça ser economicamente insustentável para a maioria dos países. Tem sido sugerido o seguimento destes doentes numa abordagem multidisciplinar. Como essas equipas multidisciplinares são também consumidoras de recursos, torna-se imperioso avaliar a sua eficácia. O objectivo deste estudo é avaliar o impacto económico e clínico da abordagem nefrológica convencional ou da equipa da consulta de baixa depuração (CBD), previamente ao início de diálise. Este estudo incluiu doentes incidentes em hemodiálise seguidos em Consulta de Nefrologia Geral vs CBD no nosso hospital, entre 2008 e 2011. Os custos foram calculados com base no sistema de capitação português introduzido em 2008. Iniciaram hemodiálise 176 doentes, 113 dos quais eram seguidos na CBD e 63 eram seguidos em Consulta de Nefrologia Geral. Não foram encontradas diferenças demográficas entre os grupos. Os doentes seguidos na CBD começaram diálise com TFG superior (10,1 vs 8.3 ml/min/1,73m2, p = 0,002), albumina mais elevada (3,8 vs 3,5 g/dl, p = 0,020), PTH mais baixa (549,7 vs 841,1 pg/ml, p = 0,008); neste grupo foi maior a proporção de doentes a iniciar diálise por acesso vascular definitivo (85,8% vs 65,5%, p = 0,002). Os parâmetros bioquímicos foram comparáveis após 6 e 12 meses, mas o custo para atingir o mesmo objectivo analítico foi muito inferior no grupo da CBD: 3737,7 vs 5087,3 euros (p = 0,005) e 6336,4 vs 8024,6 euros (p = 0,035) após 6 e 12 meses, respectivamente. Não houve diferenças na sobrevida ou morbilidade. A idade mais avançada foi associada a maior risco de hospitalização (p = 0,032) e morte (p < 0,001); um acesso vascular definitivo associou-se a menor risco de hospitalização (p=0,006) e tendencialmente de morte (p = 0,051). Melhores parâmetros bioquímicos e a presença de acesso vascular definitivo dos doentes seguidos na CBD, resultaram em menor custo durante o primeiro ano de hemodiálise.
Palavras-Chave: Consulta de baixa depuração; cuidado pré-diálise; custo-benefício; doença renal crónica; equipa multidisciplinar.
]]>INTRODUCTION
The incidence and prevalence of chronic kidney disease (CKD) has progressively risen over the last few years and, as this trend is sustained, an important health and economic issue emerges1. The projected growth in spending for the treatment of end-stage renal failure (ESRF) threatens to become unsustainable for most countries2. Prevention of ESRF is, therefore, critical. There is mounting evidence that the progression of CKD to ESRF can, in some cases, be delayed, halted or even reversed by a range of interventions3.
Chronic kidney disease is also associated with morbidity, such as renal bone disease, anaemia and cardiovascular disease, which impairs patients quality of life, but for which there are effective interventions4.
Among the many factors that influence outcome on dialysis, the initial clinical condition is of major importance and it is related to pre-dialysis care, namely specialized nephrology consultation5. Portuguese Clinical Orientation Norms, in 2011, advocated the creation of a dedicated team in each Nephrology Department, for people approaching dialysis. Information about all forms of treatment should be given and an informed choice of modality should be made. The recommended multidisciplinary renal team should, at least, incorporate a nephrologist, a nurse, a dietician and a social worker6. Kidney Disease Improving Global Outcomes (KDIGO), in 2012, also suggested that people with progressive CKD should be managed in a multidisciplinary care setting (evidence 2B). This multidisciplinary team should include or have access to dietary counselling, education and counselling about different RRT modalities, transplant options, vascular access surgery, and ethical, psychological, and social care7.
Given that multidisciplinary teams impact on health care resources, it is imperative to evaluate their effectiveness in comparison to current clinical practice8.
In 2003, our Nephrology Department created a Low Clearance Consultation, which comprises a multidisciplinary team, an educational programme, a regular clinic and laboratory follow-up of patients with chronic kidney disease presenting an estimated glomerular filtration rate under 25 ml/min/1.73 m2, adjusted to the patients individual characteristics and clinical evolution. In addition to the nephrologist in charge, a nurse and a nutritionist are always enrolled in the process of informing, educating and supporting the patient, adjusting care as kidney function deteriorates and anticipating chronic kidney disease complications. This includes a specialized education visit for treatment modality selection. A pharmacist, a psychologist and a social worker are accessed when necessary. An informed and timely choice of a dialysis technique is a priority, as well as the creation of a definitive vascular access when haemodialysis initiation is anticipated. This Low Clearance Consultation, besides providing educational leaflets, multimedia support information and group counselling, guarantees a higher number of visits per patient-year and a higher total clinic team exposure, than standard nephrology care at our Centre.
The purpose of this study was to evaluate the impact of exposure to different clinical care prior to dialysis initiation on patient outcomes and expenditure after dialysis initiation. All patients had been exposed to conventional nephrology care or low clearance clinic team care for an extended and similar period of time, assuring exclusion of the time frame referral issue.
MATERIAL AND METHODS
We included all incident dialysis patients initiating haemodialysis in Faro Hospital. This one-centre study portrays the southern region of Portugal, and the nephrology assistance to a population of 450,000. Adult patients (over 18) commencing chronic dialysis between 1st of January 2008 and 31st of December 2011 were included. The total cohort of dialysis patients during the time period was 262, but only those followed by nephrologists for more than 3 months were eligible for inclusion for this analysis, given the specific questions being addressed. Other exclusion criteria were previous kidney transplant or previous chronic dialysis treatment.
]]> The 3-month convention attempts to remove patients with late referral based on duration of time needed for education, modality selection and access creation and assessment in a non-urgent manner.Patients were categorized according to the nephrology care previous to dialysis initiation: attending a multidisciplinary-based education and follow-up programme, addressed as LCC (low clearance care); or receiving standard nephrologist care (SNC). All nephrologists had the same opportunity to access facilities and personnel of the multidisciplinary clinic for their patients. Patients right to choose to maintain the existing bound nephrologist/patient or to attend LCC was respected. All patients gave informed consent and the local ethics committee approved the study.
After dialysis initiation, patients were transferred the haemodialysis clinic of the area. For the economic analysis, this clinic was adherent to the capitation system for dialysis payment, which is described in detail elsewhere2. In brief, besides the dialysis treatment, this entails the laboratory and imaging tests, all medication for the treatment of anaemia, bone mineral disease, nutrition and cardiovascular co-morbidities, intradialytic intravenous antibiotics and, since 2011, vascular access management. In this setting, the costs per patient for all of the above mentioned medication (such as vitamin D, phosphate binders, cinacalcet, iron, erythropoietin-stimulating agents, antihypertensive pills and potassium binders) were known.
Data collection and measurements
Data were collected from all patients at the time of dialysis initiation. Baseline data included demographics, diabetic status and cardiovascular disease, date of first nephrology referral and presence of a functioning definitive vascular access (arteriovenous fistula or prosthesis). Serial laboratory data were collected at the time of dialysis initiation and monthly until 12 months of follow-up. The estimated glomerular filtration rate (GFR) at dialysis initiation was attained using the four variable (abbreviated) Modification of Diet in Renal Disease (MDRD) study equation9.
Serial medication costs were collected on all patients monthly until 12 months of follow-up. Patient status (on dialysis, deceased, transplanted, discontinued treatment, or moved), causes of death, number and duration of hospitalizations were also obtained at the end of the study period for each cohort.
Statistical analysis
The statistical analysis was performed using SPSS software for Windows (version 20.0; Chicago, USA).
Results are presented as mean ± standard deviation for continuous variables and as frequency and percentages (n, %) for categorical variables. P-values < 0.05 were considered statistically significant. For comparison between groups, the students t-test or Wilcoxon rank-sum test, depending on distribution, and chi-squared test were used for continuous parametric variables and categorical variables, respectively. We used a binary logistic regression model to evaluate the risk of hospitalization. As the dependent variable, we used hospitalization (yes/no) and, as independent variables, age, gender, GFR (MDRD), type of vascular access, type of nephrology follow-up, presence of diabetes and cardiovascular disease.
Survival on dialysis was examined using the KaplanMeier method and survival by clinic attendance was compared using the log-rank test. Patients were censored at transplant, moving away, and end of study period. Cox proportional hazard modeling was also used to examine hazard ratios for death as outcome. In this model, we introduced as independent variables age, gender, GFR (MDRD), type of vascular access, type of nephrology follow-up, presence of diabetes and cardiovascular disease.
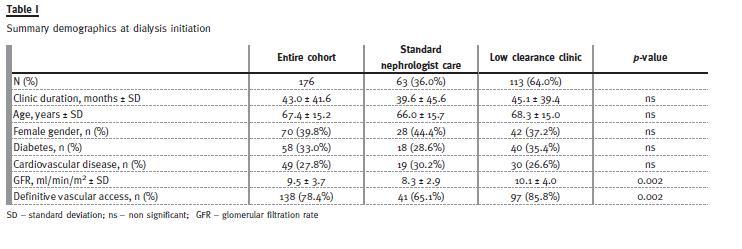
]]> RESULTSWe included a total of 176 patients, with an average of 43 months of nephrology care. Table I presents the demographic data at dialysis initiation, and comparisons between those patients seen in LCC vs. standard nephrology care. These study cohort populations are similar in demographics to those described in national registries from Portugal10.
Follow-up before dialysis initiation, age, gender, presence of diabetes or cardiovascular disease were not statistically different between groups. Patients followed at the LCC initiated dialysis with higher eGFR (p = 0.002). Regarding vascular access, the proportion of patients that started dialysis with fistula or vascular graft was significantly higher in the LCC group (p = 0.002) (Table I).
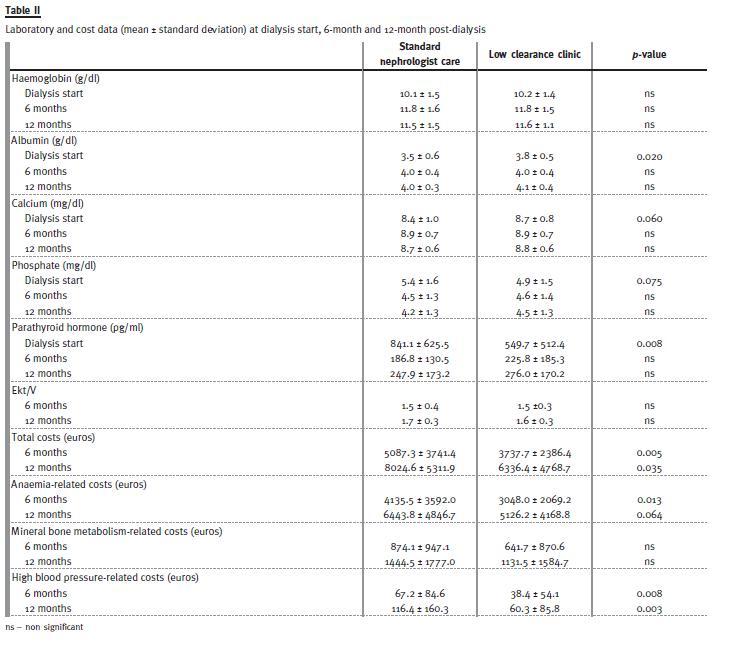
Table II describes the laboratory data at dialysis initiation in both groups. There were significant differences regarding albumin (3.5 vs. 3.8 g/dl, p = 0.02) and PTH (841.1 vs. 549.7 pg/ml, p = 0.008). Although a statistical significance was not found, a trend of higher calcium and lower phosphate levels was found in patients attending the LCC. All these parameters became similar over the course of dialysis, with no analytical differences present after 6 months.
Regarding cost analysis, total costs were higher in the group followed with standard nephrology care, 6 months after dialysis initiation (5087.3 vs. 3737.7 euros, p = 0.005) and 12 months after dialysis initiation (8024.6 vs. 6336.4 euros, p = 0.035), to attain the same clinical target (evaluated by biochemical parameters). These higher costs were mainly due to higher expenditure with anaemiarelated medication at 6 months (4135.5 vs. 3048.0, p = 0.013) and 12 months (6443.8 vs. 5126.2, p = 0.0064), respectively. This difference tends to diminish within the first dialysis year, but it is still noticed after this time, revealing an actual difference of nearly 1700 euros per patient more expensive in the group not exposed to the LCC. There was also a sustained difference in the cost of anti-hypertensive drugs prescribed, although equivalent clinical outcome could not be ascertained with the data available.
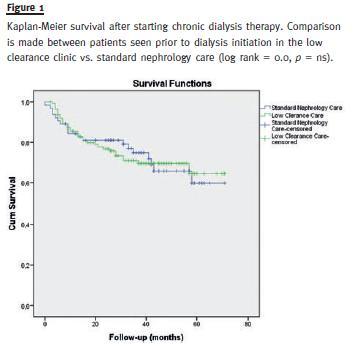
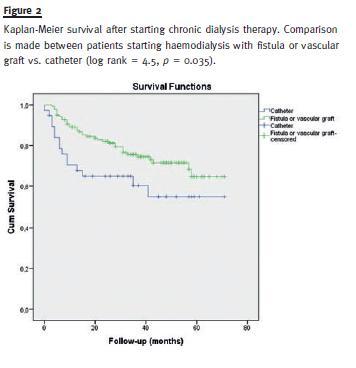
Patients were followed for a mean of 33 months after dialysis start. The analysis of hospitalization days (excluding the initial hospital stay, if dialysis was initiated during a hospitalization) showed that LCC patients had fewer hospital stays (9.2 ± 17.9 days vs. 6.8 ± 11.4 days), but this difference was not significant, probably due to a high dispersion of the data. In the LCC group, eight patients were transplanted, nine were lost to follow-up or transferred and 32 died. In the standard nephrology care group, five patients were transplanted, three were lost to follow-up or transferred and 19 died. Kaplan Meier analysis was used and Fig. 1 demonstrates the difference in survival after dialysis initiation, between the groups considered. There was no statistically significant survival advantage of those attending the LCC over those patients in the standard nephrology cohort. Figure 2 shows a survival analysis comparing those patients starting haemodialysis with a permanent vascular access vs. initiating with a catheter (log rank = 4.5, p = 0.035).
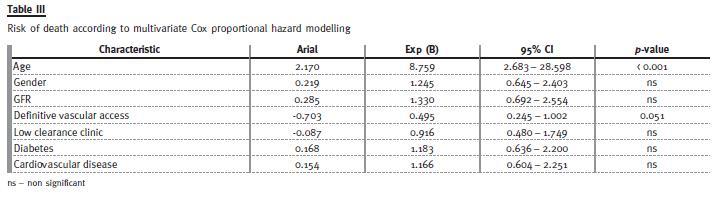
We analysed the risk of death using the Cox proportional hazard modelling. As independent variables, we included age (< 65 and > 65 years), gender, GFR (MDRD), type of vascular access (graft or arteriovenous fistula vs. catheter), type of nephrology followup and presence of diabetes or cardiovascular disease. Only age (over 65) influenced the survival (p < 0.001). The initiation of dialysis with a definitive vascular access (graft or arteriovenous fistula) showed a trend to be associated with greater survival (p = 0.051) (Table III).
]]> Despite the absence of a statistical significance for risk of death, the presence of a definitive vascular access did impact the hospitalization risk (p = 0.006), with a protective role. Age (over 65) is also correlated with higher hospitalization (p = 0.032) (Table IV).DISCUSSION
The authors describe their 10 years experience in multidisciplinary team care, but in this work they used only data from patients starting dialysis after 2008, when the Portuguese capitation system was introduced2.
It is generally accepted, but not proven, that the multidisciplinary approach is the best way to manage the complex needs of patients approaching end-stage renal failure11. Several studies have highlighted the benefits of early referral to pre-dialysis services and to multidisciplinary teams, such as better clinical variables at the start of dialysis8,11,12 and also better survival rate8,11. Before further discussion, it is important to emphasize that there was no difference between the two groups (low clearance or standard nephrology), regarding age, gender, duration of nephrology follow-up, presence of diabetes or cardiovascular disease. Despite these similar demographic characteristics and co-morbidities, the LCC group started dialysis with a trend in better calcium and phosphate control, with lower PTH (p = 0.008), and higher albumin levels (p = 0.02). This fact can be due to several factors: a higher GFR at the time of dialysis start, the dieticians educating role, a higher exposure to health care professionals and respective corrective measures or, also, a subsequent higher self-awareness of the disease and compliance with treatments.
After initiation of dialysis, these differences disappeared, as presented in 6-month and 12-month evaluations, with both groups attaining the biochemical objectives advocated by the international guidelines13,14 and by the capitation model adopted in Portugal2. Notwithstanding, the group followed by standard nephrology care needed more medication to achieve the same targets, with greater costs at 6-month and 12-month analysis. Concerning mineral bone disease medication costs, the difference was not statistically significant, possibly due to dispersion of the variables. This could also be explained by the fact that dialysis improves phosphate control. The equivalent initial haemoglobin levels in both groups would not predict a different expenditure when comparing prescriptions, but we do not know the dosage of iron or erythropoietin-stimulating agents prescribed before dialysis start. The initial inflammatory state of these patients, determined by C-reactive protein, was equivalent.
Another important fact presented in the cost analysis is the difference in the prescribed antihypertensive medication, remaining more costly in the group that received standard nephrology care.
The cost-effectiveness in this case cannot be ascertained, because initial prevalence of high blood pressure is not known due to the lack of data.
However, because we have the same therapeutic target for all patients, this could be interpreted as better nutritional behaviour (with a low salt diet) or a higher compliance to dry weight prescription, both results of a more intensive and multidisciplinary follow-up/education previously.
Harris et al. showed that an intensive multidisciplinary management approach did not appear to offer any significant advantage in terms of mortality rate, as compared with standard nephrology care12.
In fact, our study shows no mortality or morbidity (analysed as hospitalization days) difference between the groups. Instead, it shows a predominant effect of the vascular access on morbidity and mortality. Current guidelines suggest that up to 12 months in advance of dialysis initiation, specialized nephrology consultation should be warranted7, as a 6-month time frame may be needed for adequate vascular access maturation and optimization of care15. Nevertheless, even using this 3-month cutoff, 65.1% of patients referred to standard nephrology care started dialysis using a definitive vascular access, but 85.8% of patients belonging to the LCC group started dialysis with a definitive vascular access (p = 0.002). Most of the effort of the LCC team is directed towards the patients informed and timely choice of a dialysis technique, in order to guarantee a functioning definitive vascular access when haemodialysis initiation is anticipated. The avoidance of catheters has been recognized to be beneficial in several studies16,17 and is recognized as good clinical practice15. This constitutes the main advantage and objective of the multidisciplinary team, as it has been proven to reduce morbidity and mortality18,19. The savings obtained with LCC are mainly attributed to less ESA consumption, and this can in fact be a consequence of an LCC, as its main advantage is the higher percentage of patients starting HD with a definitive blood access.
]]> Catheter usage is known to be associated with chronic inflammation and this can in turn be a reason for higher ESA consumption. This study also demonstrates a reduced number of hospitalization days in patients starting haemodialysis with a definitive vascular access (p = 0.006), and a trend to reduced mortality (p = 0.051) regardless of the type of pre-dialysis follow-up. The costs with these hospitalizations were not calculated, but came as an extra expense to the group with standard nephrology care.In summary, better biochemical parameters and the presence of a definitive vascular access were the major advantages of the LCC. Mortality should be influenced by these initial characteristics. However, the quick biochemical recovery shown, attaining equal analytical evolution in less than 6 months, probably attenuated these differences, and the mortality was similar in both groups. This work shows a big and sustained difference in costs, supporting the LCC, with an economic advantage that is still remarkable at least after one year on haemodialysis.
The convergence point was not found, as further data was not available. This ends up strengthening Heatleys words early and timely education and preparation is never a wasted commodity11 .
A major flaw of our work was its retrospective nature and the possibility of a selection bias, despite equal opportunities to be referred to the clinic. In a time of economic constraints, a prospective study is needed, to confirm that an LCC with a multidisciplinary team will serve as a way to save resources.
References
1. Van Dijk PC, Jager KJ, De Charro F, et al. and the ERA-EDTA registry. Renal replacement therapy in Europe: the results of a collaborative effort by the ERA-EDTA registry and six national or regional registries. Nephrol Dial Transplant 2001; 16(6):1120-1129. [ Links ]
2. Ponce P, Marcelli D, Guerreiro A, et al. Converting to a capitation system for dialysis payment the Portuguese experience. Blood Purif 2012; 34(3-4): 313-324. [ Links ]
]]>3. Ruggenenti P, Schieppati A, Remuzzi G. Progression, remission, regression of chronic renal diseases. Lancet 2001; 357(9268):16011608. [ Links ]
4. Roderick P, Jones C, Tomson C, Mason J. Late referral for dialysis: improving the management of chronic renal disease. QJM 2002; 95(6):363370. [ Links ]
5. Peña JM, Logroño JM, Pernaute R, Laviades C, Virto R, Vicente de Vera C. La referencia tardía al nefrólogo influye en la morbi-mortalidad de los pacientes en hemodiálisis. Un estudio provincial. Nefrología 2006; 26(1):84-97. [ Links ]
6. Norma da Direcção Geral de Saúde, nº 017/2011 de 28/09/2011, www.dgs.pt [ Links ]
7. KDIGO (Kidney Disease: Improving Global Outcomes) - Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int 2013; 31. [ Links ]
8. Curtis BM, Ravani P, Malberti F, et al. The short- and long-term impact of multi-disciplinary clinics in addition to standard nephrology care on patient outcomes. Nephrol Dial Transplant 2005; 20(1):147154. [ Links ]
9. Levey AS, Coresh J, Greene T, et al. with the Chronic Kidney Disease Epidemiology Collaboration. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med 2006; 145(4):247-254. [ Links ]
10. http://www.spnefro.pt/comissoes_gabinetes/gabinete_de_registo_DRT.asp Relatórios Anuais 2012, accessed on 10th December 2013. [ Links ]
11. Heatley SA. Optimal referral is early referral. Perit Dial Int 2009; 29(Suppl 2):128-131. [ Links ]
12. Harris LE, Luft FC, Rudy DW, Kesterson JG, Tierney WM. Effects of multidisciplinary case management in patients with chronic renal insufficiency. Am J Med 1998; 105(6):464471. [ Links ]
13. KDIGO (Kidney Disease: Improving Global Outcomes) - clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). CKD-MBD Work Group et al. Kidney Int Suppl 2009; 113:S1-130. [ Links ]
14. KDIGO (Kidney Disease: Improving Global Outcomes) - Clinical Practice Guidelines for Anemia Management in Chronic Kidney Disease. Kidney Int Suppl 2012; 2: 279-335. [ Links ]
15. KDOQI Clinical Practice Guidelines for Vascular Access. Am J Kidney Dis. 2006; 48 (Suppl 1): S176-S247. [ Links ]
16. Woods JD, Turenne MN, Strawderman RL, et al. Vascular access survival among incident hemodialysis patients in the United States. Am J Kidney Dis 1997; 30(1): 50-57. [ Links ]
17. Lukowsky LR, Kheifets L, Arah OA, Nissenson AR, Kalantar-Zadeh K. Patterns and predictors of early mortality in incident hemodialysis patients: new insights. Am J Nephrol 2012; 35(6):548-558. [ Links ]
18. Ng LJ, Chen F, Pisoni RL, et al. Hospitalization risks related to vascular access type among incident US hemodialysis patients. Nephrol Dial Transplant 2011; 26(11):3659-3666. [ Links ]
19. Lorenzo V, Martn M, Rufino M, Hernández D, Torres A, Ayus JC. Predialysis nephrologic care and a functioning arteriovenous fistula at entry are associated with better survival in incident hemodialysis patients: an observational cohort study. Am J Kidney Dis 2004; 43(6):999-1007. [ Links ]
Drª Anabela Malho Guedes
Department of Nephrology, Hospital de Faro,
Rua Leão Penedo, 8000 Faro, Portugal.
E-mail: anabelamalho@hotmail.com
]]> Conflict of interest statement: Anabela Malho Guedes, Ana Paula Silva, Carlos Gonçalves, Elsa Morgado, Patrícia Mendes, Isilda Bexiga, Viriato Santos, Idalécio Bernardo and Pedro Leão Neves are employees of Nephrocare.
Received for publication: 21/10/2014
Accepted in revised form: 11/02/2015
]]>{kind=link}