{kind=link}
When acute interstitial nephritis has systemic involvement: TINU syndrome
Quando a nefrite intersticial aguda tem atingimento sistémico: síndrome de TINU
Ana Pimentel1, Ana Cabrita1, Andre Fragoso1, Teresa Jeronimo1, Joana Vidinha1, Sandra Sampaio1, Idalecio Bernardo1, Fernanda Carvalho2, Pedro Leao Neves1
1 Department of Nephrology. Centro Hospitalar do Algarve, Faro, Portugal.
2 Renal Morphology Laboratory, Department of Nephrology. Hospital de Curry Cabral, Lisboa, Portugal.
]]> ABSTRACT
Tubulointerstitial nephritis is commonly related with the use of medication or the presence of infection. When uveitis precedes, follows or simultaneously occurs, a distinct and rare syndrome develops as part of the systemic illness. The initial investigation of tubulointerstitial and uveitis syndrome should exclude other systemic diseases that affect the eye and kidney. The diagnosis must include histopathological and clinical findings. The clinical course and treatment may rely on immunomodulatory agents. Case: 24-year old obese male admitted with rapidly progressive renal insufficiency without any identified precipitant factor that responded well to intravenous metilprednisolone. Renal biopsy revealed acute tubulointerstitial nephritis. Uveitis appeared when systemic steroids were tapered.
Key-Words: Steroids; tubulointerstitial nephritis; uveitis.
RESUMO
A nefrite tubulointersticial está frequentemente associada ao uso de fármacos ou à presença de infeção. Quando há uveíte que precede, acompanha ou surge posteriormente à nefrite, existe confirmação de uma distinta e rara síndrome com envolvimento sistémico. A investigação inicial da síndrome de nefrite intersticial e uveíte inclui a exclusão de outras doenças sistémicas com envolvimento ocular e renal. O diagnóstico baseia-se em achados histopatológicos e clínicos. A própria evolução clínica e o tratamento podem vir a depender de agentes imunomoduladores. Caso: Homem obeso de 24 anos, internado por insuficiência renal rapidamente progressiva, sem nenhum factor precipitante identificado, que respondeu favoravelmente a metilprednisolona endovenosa. A biopsia renal revelou nefrite tubulointersticial aguda. Aquando do desmame da corticoterapia sistémica desenvolveu uveíte.
Palavras -Chave: Corticoterapia; nefrite tubulointersticial; uveíte.
INTRODUCTION
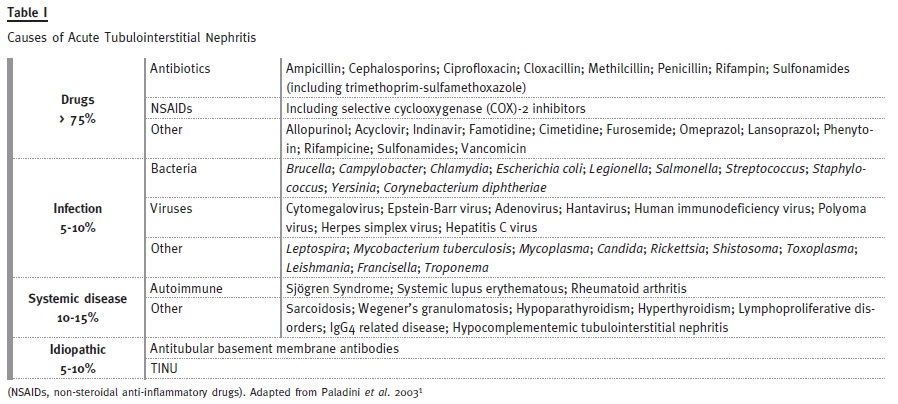
Tubulointerstitial nephritis (TIN) is most frequently related with the use of medication, infection or autoimmune diseases1 (Table I) and rarely presents other systemic involvement. About 15% of biopsies in acute kidney injury reveal TIN2,3. When uveitis precedes, follows or simultaneous occurs with nephritis, a distinct and rare syndrome (TINU) develops as a part of the systemic illness. Several unspecific signs can be present, such as fever, abdominal pain or anaemia, and it is three times more common in women4.
]]> Although TINUs physiopathology is still not well understood, the clinical course and treatment may rely on immunomodulatory agents to prevent and treat inflammation. Renal involvement is diversified, ranging between urinary findings such as sterile pyuria, haematuria and subnephrotic proteinuria to mild or severe renal insufficiency. Most adult patients have incomplete recovery5.CASE REPORT
A 24 -year old Caucasian, obese (mean BMI 32.2 kg/m2) male presented with nausea, fatigue and vomiting with a 3-day history of diarrhoea and right flank pain for which he was given non-steroidal anti-inflammatory drugs (NSAIDs). He was then admitted to the nephrology department with rapidly progressive renal insufficiency. The patient had no relevant past medical or family histories.
On admission he presented normal physical examination and was afebrile and normotensive. Laboratory tests conducted at the hospital showed haemoglobin 12.6g/dL, leucocytes 13300μL, platelet count 455000 μL, blood urea nitrogen of 22mg/dL, serum creatinine 3.55mg/dL, C reactive protein (CPR) 139mg/L, urinalysis with proteins ++, blood + and no dysmorphic erythrocytes or eosinophils. Blood and urine cultures were drawn and he was started on saline 0.9% IV drip and empiric antibiotics (amoxycillin and clavulanic acid) due to fever and elevation of inflammatory laboratory parameters of unknown origin. Afterwards blood and urine bacteriologic cultures from admission revealed to be sterile. Further laboratory tests showed normal serum calcium (9 mg/dL), phosphorus (3.7mg/dL), sodium (135mmol/L), potassium (4mmol/L), chloride (100mmol/L), bicarbonate (25mmol/L), fasting glucose (84mg/dL) and parathyroid hormone (120 pg/mL).
On the 5th day of admission, serum creatinine rose up to 5.63 mg/dL and metilprednisolone IV was given for four days, 500mg/day improving serum creatinine to 3.81mg/dL and then prednisolone 60mg/ day was given orally. Inflammatory biomarkers remained elevated and amoxycillin and clavulanic acid was replaced with piperacillin and tazobactan. At the time, twenty-four hour urinalysis indicated 419mg proteinuria. The immune assays performed were normal or negative for anti-nuclear antibodies (ANA), anti-double stranded DNA antibodies (AntidsDNA), anti-neutrophil cytoplasmic antibodies (ANCA), anti-glomerular basal membrane (GBM), rheumatoid factor (RF), anti-hepatitis C virus (HCV), anti-hepatitis B virus (HBV) and human immunodeficiency virus (HIV) 1 and 2 antibodies. Renal ultrasound was unremarkable. Epstein Barr virus serology indicated previous exposure to the virus with positive IgG antibodies and viral capsid antigen (VCA) IgG antibodies, without positive VCA IgM antibodies.
In the absence of clinical features such as granulomatous lesions and lymphadenopathies with no pulmonary involvement in thoracic X-ray and normal range serum angiotensin conversion enzyme (ECA), tuberculosis and sarcoidosis were excluded. There were no clinical signs for other autoimmune disease, such as arthralgia, skin involvement or any allergic reactions previous to this episode. The patient was discharged twelve days later, asymptomatic with improved renal function under steroids. Renal biopsy was postponed, even tough infection was excluded; there was underlined systemic inflammatory reaction at the time, as well as all technical difficulties secondary to the patients phenotype.
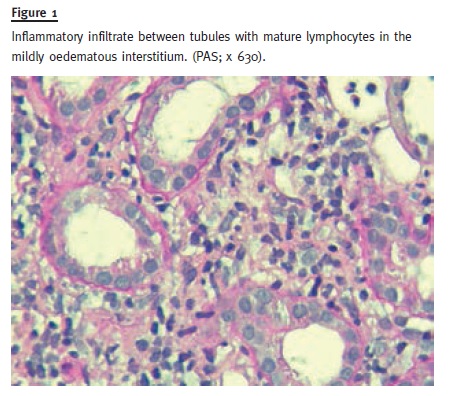
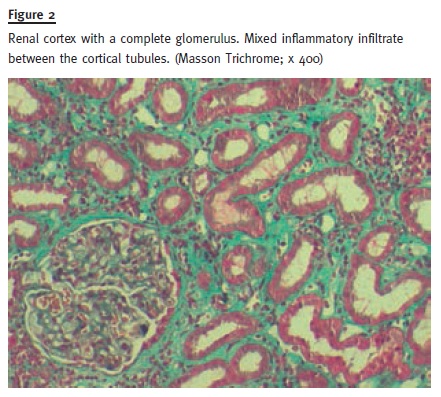
The patient was readmitted a few months later maintaining improved renal function with a serum creatinine of 1.47mg/dL, C-reactive protein (CRP) 15mg/L, medicated with 20mg of prednisolone per day. Renal biopsy was then performed and revealed signs of acute tubulointerstitial nephritis with normal glomeruli and interstitial oedema with cellular infiltration, mainly lymphocytes. Neither granulomatous lesions nor fibrosis or eosinophils were found. Immunofluorescence was negative. (Figs.1 and 2)
]]> Six months after being admitted, and while tapering prednisolone to 15mg per day, he started presenting burning sensation, photophobia and redness in both eyes, accompanied by decreased visual acuity.
The ophthalmologist affirmed to be a non-granulomatous anterior uveitis and added topical steroids to the existing systemic steroid therapy. Two weeks after the uveitis improved.
The patient is still being medicated with prednisolone 2.5md/day and ramipril 1.25mg/day, as well as topic ocular steroids. He presents normal renal function with serum creatinine of 1.15mg/dL and 306mg/24 hour proteinuria. He is aware of the possibility of frequent relapse and he maintains a regular followup with the ophthalmologist.
DISCUSSION
The TINU is a rare syndrome with an estimated prevalence between 2% in tertiary uveitis centres, up to 28% of TIN biopsies in Chinese adults5,6. Usually nephritis precedes uveitis in 65% of the cases, as the case presented before7. New reports indicate that TINU is underestimated since it can be subclinical in patients presenting isolated uveitis8.
Autoimmune diseases, such as rheumatoid arthritis4, sacroileiitis9 and hyperthyroidism10, as well as systemic infections and the use of several drugs have been described prior to the appearance of TINU syndrome4. These insults act like triggers and seem to cause exuberant immune reactions, sufficient to cause an impact on the kidney. In this particular case, although the presentation of unspecific systemic features as fatigue, flank pain and fever, our patient had no other signs of infection at admission. No infectious agents were isolated and serological survey for most common agents of TIN was negative, compatible with the usual clinical presentation of TINU syndrome and inherent systemic inflammation that commonly last longer than 2 weeks. Empiric antibiotics were given to the patient when he was already admitted for rapidly progressive renal insufficiency.
Although he had high systemic inflammatory markers, there were no other immunological or clinical signs, compatible with autoimmune diseases.
At the time, since drug induced interstitial nephritis could always be a possibility and renal function kept worsening, IV metilprednisolone 500mg/day was started for four days, improving renal function.
Although there are no randomized trials or prospective studies comparing placebo to steroid therapy studying dose and treatment duration, patients with progressive renal insufficiency are typically treated with prednisone at the dose of 1mg/Kg/day until 40 to 60mg/day for 3 to 6 months and then slowly tapered11. In our case, similarly to the one presented by Sinnamon et al. 12 when reducing the course of oral prednisolone (in their case 0.8 mg/kg/day tapered to zero over 18 weeks) there was relapse of anterior bilateral uveitis two weeks later, requiring reinstitution of oral prednisolone at 10 mg daily.
Ambiguity in the general therapeutic approach is, once more, related to the fact that TINUs physiopathology is not well clarified. Both humoral and cell-mediated immunity seem to be implied, with lymphocyte T having a more prominent role.
]]> Autoantibodies directed against tubular and ocular antigens may also be implicated13, as well as some determined HLA profiles (HLA -DQA1*01, HLA -DQB1*05, and HLA -DQB1*01)14. The TINU syndrome has also been associated with positive antineutrophil cytoplasmic antibody (ANCA), antinuclear antibody (ANA), rheumatoid factor (RF) and hypocomplementemia15,16, none of the latter features was present in our patient.In TINU syndrome patients, renal biopsy presents distal tubules that stain strongly with anti-Krebs von den Lunge-6 (KL -6) antibody, a human glycoprotein, suggesting that the elevated KL-6 levels may reflect underlying renal affection17. Pepple et al. highlight the importance of urinary β2-microglobulin testing in the paediatric patient uveitis population because extreme elevations in urinary β2 -microglobulin may be used with concomitant renal biopsy to differentiate between TINU and sarcoidosis18. Autoantibodies against modified C -reactive protein (mCRP -Ab) were also measured and seem to be useful in predicting late-onset uveitis TINU syndrome19.
The diagnosis of TINU requires the presence of TIN and uveitis and the exclusion of other systemic disease directly causing the same features. Li et al. showed that late-uveitis TINU was clinically and pathologically indistinguishable from drug-induced TIN at biopsy5. Mandeville et al. proposed several criterions for more accurate diagnosis4. Our patient has a definite TINU syndrome hence fulfilment of the three criteria, acute TIN diagnosed 1) histopathologically 2) clinically and 3) the presence of typical uveitis.
The three criteria for the clinical diagnosis for acute TIN are abnormal renal function, abnormal urinalysis and systemic illness lasting two weeks or more.
Histopathologically, most patient biopsies reveal diffuse tubulointerstitial inflammation, with cellular infiltration predominantly T lymphocytes, accounting approximately for 48% of all inflammatory cells, but it is also possible to observe B lymphocytes (12%), plasma cells (11%) monocytes/macrophages (24%), and neutrophils (6%)5. Eosinophils are also occasionally seen. Fibrosis is usually < 25% of the interstitial area and immunofluorescence staining is commonly negative for Ig or complement.5
The differential diagnosis should include other systemic diseases that involve the eye and kidney like sarcoidosis, Wegeners granulomatosis, Sjögren syndrome, systemic lupus erythematous, rheumatoid arthritis, IgG4 -related disease and infectious diseases, such as tuberculosis. Besides the previous investigation, it should also contemplate excluding Behçets disease and systemic sclerosis20.
The TINU syndrome should be considered in cases of idiopathic acute interstitial nephritis and in those with the sudden onset of anterior uveitis. In TINU syndrome, uveitis is typically non-granulomatous, anterior and bilateral. Cycloplegic agents are used to avoid the development of posterior synechiae12.
Patients with uveitis should get at least a urinalysis with the purpose of identifying any signs of proximal or distal tubular dysfunction as polyuria, nocturia, aminoaciduria, normoglycaemic glycosuria, phosphaturia and acidification defects. Laboratory findings may also include eosinophilia, normochromic normocytic anaemia, slightly abnormal liver function tests, none of which were present in our patient, only high CRP5.
In this case, there was complete recovery of the renal function, but renal prognosis is variable ranging from complete or incomplete recovery to persistent chronic kidney disease in some cases12.
Although topical and systemic steroids are successfully used to treat uveitis, it is likely to recur and relapse. There are reports of limited number of patients using steroid-sparing immunosuppressant agents, such as azathioprine, methotrexate21, cyclosporine22 and mycophenolate mofetil23,24, rarely biologic agents have been used. Tumour necrosis factor (TNF) blockers have been demonstrated to be effective in the treatment of systemic and ocular inflammatory diseases. Adalimumab seemed safe and effective also in refractory uveitis patients, although further studies are necessary to check its effect in refractory TINU, indicating a possible role of TNF in TINU pathogenesis25,26.
]]> In conclusion, TINU remains a diagnosis of exclusion based on the presence of uveitis and acute tubulointerstitial nephritis turning renal biopsy and the absence of other disease that could explain theses two findings mandatory. In some cases, previous infection, use of medication or autoimmune disease may have an important role in the incidence of TIN and TINU. Ocular manifestations can recur and may need prolonged treatment, therefore, ophthalmological follow-up is warranted. The incidence of TINU syndrome may be increasing and the epidemiology probably is changing too, revealing a growing prevalence in men and the elderly12. Due to its unpredictable clinical course, ranging from limited symptoms to chronic kidney and eye disease, it is deemed necessary to have in mind the possibility of every TIN and every uveitis to evolve into a TINU syndrome. Further randomized, prospective and multi-centred studies are necessary to have consensual therapeutic approach.
References
1. Paladini A, Venturoli V, Mosconi G, Zambianchi L, Serra L Valletta E. Tubulointerstitial nephritis and uveitis syndrome in a twelve-year-old girl. Case Reports in Pediatrics. Volume 2013, Article ID 652043, 4 pages.http://dx.doi.org/10.1155/2013/652043 [ Links ]
2. Michel DM, Kelly CJ. Acute interstitial nephritis. J Am Soc Nephrol 1998;9(3):506-515. [ Links ]
3. Clarkson M, Giblin L, OConnell F et al. Nephrol Dial Transplant. 2004;19:2278-2783. [ Links ]
4. Mandeville JT, Levinson RD, Holland GN. The tubulointerstitital nephritis and uveitis syndrome. Surv Ophtalmol 2001;46(3):195-208. [ Links ]
]]>5. Li C, SU T, Chu R, Li X, Yang L. Tubulointerstitial nephritis and uveitis in Chinese adults. Clin J Am Soc Nephrol 2014;9(1)21-28. [ Links ]
6. Kump LI, Cervantes-Castañeda RA, Androudi SN, Foster CS. Analysis of pediatric uveitis cases at a tertiary referral center. Ophthalmology 2005;112(7):1287 -1292. [ Links ]
7. Mackensen F, Smith JR, Rosenbaum JT. Enhanced recognition, treatment and prognosis of tubulointerstitial nephritis and uveitis syndrome. Ophthalmology 2007;114(5):995-999. [ Links ]
8. Timmermans SA, Huitema JJ, Wirtz JJ. Keep an eye out for tubule-interstitial nephritis. Neth J Med 2013;71(10):523-525. [ Links ]
9. Cigni A, Soro G, Faedda R, et al. A case of adult-onset tubulointerstitial nephritis and uveitis (TINU syndrome) associated with sacroileitis and Epstein -Barr virus infection with good spontaneous outcome. Am J Kidney Dis 2003;42(3): E4 -E10. [ Links ]
]]>10. Ebihara I, Hirayama K, Usui J, et al. Tubulointerstitial nephritis and uveitis syndrome associated with hyperthyroidism. Clin Exp Nephrol 2006;10(3):216 -221. [ Links ]
11. Mabrouk AR, Bensalam L, Atik A. TINU syndrome, a case report and literature review. Urol Nephrol Open Access J 2015;2(1):00026. DOI 10.15406/unoaj.2015.02.00026. [ Links ]
12. Sinnamon KT, Courtney AE, Harron C, ORourke DM, Mullan RN. Tubulointerstitial nephritis and uveitis (TINU) syndrome: epidemiology, diagnosis and management. NDT Plus 2008;1(2):112-116. [ Links ]
13. Abed L, Merouani A, Haddad E, Benoit G, Oligny LL, Sartelet H. Presence of autoantibodies against tubular and uveal cells in a patient with tubulointerstitial nephritis and uveitis (TINU) syndrome. Nephrol Dial Transplant 2008;23(4):1452-1455. [ Links ]
14. Mackensen F, David F, Schwenger V, et al. HLA-DRB1*0102 is associated with TINU syndrome and bilateral, sudden-onset anterior uveitis but not with interstitial nephritis alone. Br J Ophthalmol 2011;95(7):971-975. [ Links ]
]]>15. Simon AH, Alves-Filho G, Ribeiro-Alves MA. Acute tubulointerstitial nephritis and uveitis with antineutrophil cytoplasmatic antibody. Am J Kidney Dis 1996;28(1):124-127. [ Links ]
16. Conz PA, Milan M, Bragantini L, La Greca G, Bevilacqua PA. TINU syndrome associated with reduced complement levels. Nephron 2001;89(3):340 -341. [ Links ]
17. Kase S, Kitaichi N, Namba K, et al. Elevation of serum Krebs von den Lunge -6 levels in patients with tubulointerstitial nephritis and uveitis syndrome. Am J Kidney Dis 2006;48(6):935-941. [ Links ]
18. Pepple KL, Lam DL, Finn LS, Van Gelder R. Urinary β2 -microglobulin testing in pediatric uveitis: a case report of a 9 -year -old boy with renal and ocular sarcoidosis. Case Rep Ophthalmol 2015;6(1):101 -105. [ Links ]
19. Tan Y, Yu F, Qu Z, et al. Modified C-reactive protein might be a target autoantigen of TINU syndrome. Clin J Am Soc Nephrol 2011;6(1):93 -100. [ Links ]
]]>20. Izzedine H. Tubulointerstitial nephritis and uveitis syndrome (TINU): a step forward to understanding an elusive oculorenal syndrome. Nephrol Dial Transplant 2008;23(4):1095-1097. [ Links ]
21. Hudde T, Heinz C, Neudorf U, Hoeft S, Heiligenhaus A, Steuhl KP. [Tubulointerstitial nephritis and uveitis (TINU syndrome) comorbidity and complications in four patients]. Klin Monbl Augenheilkd 2002;219(7):528-532. [ Links ]
22. Lee J, Kim H, Sung S, Lee S. A case of tubulointerstitial nephritis and uveitis syndrome with severe immunologic dysregulation. Pediatr Nephrol 2005;20(12):1805-1808. [ Links ]
23. Neilson EG, Farris AB. Case records of Massachussets General Hospital. Case 21-2009. A 61 -year -old woman with abdominal pain, weight loss, and renal failure. N Engl J Med 2009;361(2):179-187. [ Links ]
24. Preddie DC, Markowitz GS, Radhakrishnan J, et al. Mycophenolate mofetil for the treatment of interstitial nephritis. Clin J Am Soc Nephrol 2006;1(4):718-722. [ Links ]
]]>25. Suhler EB, Lowder CY, Goldstein DA, et al. Adalimumab therapy for refractory uveitis: results of a multicentre, open -label, prospective trial. Br J Ophthalmol 2013;97(4): 481-486. [ Links ]
26. Häusler U, Guminski B, Helmchen U, Kisters K, Heinz C, Braun J. [Tubulointerstitial nephritis with uveitis (TINU) syndrome. A relatively rare rheumatological differential diagnosis with unexplained uveitis]. Z Rheumatol 2013;72(4):393 -397. [ Links ]
Drª Ana Pocinho Pimentel
Department of Nephrology
Centro Hospitalar do Algarve Unidade de Faro
Rua Penedo Leão, 8000-386 Faro, Portugal.
]]> E-mail: anappimentel@gmail.com
Conflict of interest statement: None declared.
Received for publication: 04/07/2015
Accepted in revised form: 25/10/2015
]]>