Obesity‑related nephropathy in children the need for greater awareness
Liane Correia‑Costa1,2,3, Ana Azevedo1,4, Alberto Caldas Afonso1,2,3
1 EPIUnit Institute of Public Health, University of Porto, Porto, Portugal;
2 Division of Pediatric Nephrology, Integrated Pediatric Hospital, Centro Hospitalar São João, Porto, Portugal;
3 Department of Pediatrics, Faculty of Medicine, University of Porto, Porto, Portugal;
4 Department of Clinical Epidemiology, Predictive Medicine and Public Health, Faculty of Medicine, University of Porto, Porto, Portugal.
]]> Correspondence to:
Fat accumulation is known to lead to the development of several cardiovascular risk factors and metabolic disturbances, such as hypertension, dyslipidaemia and insulin resistance. In children, we know from several longitudinal studies that obesity and its metabolic and cardiovascular consequences start early in life and accompany the obese child into adulthood, implying a higher risk of diabetes, hypertension and adverse cardiovascular events.
More recently, in adults, evidence has emerged that obesity might also play a role in the risk of kidney disease, independently of diabetes. There has been a dramatic rise in the prevalence of end‑stage renal disease, which has more than doubled in the past decade, and which has occurred in parallel with the increased prevalence of obesity. In 2014, the Global Burden Disease Study reported that the worldwide prevalence of overweight and obesity rose by 27.5% for adults and 47.1% for children between 1980 and 20131 and while in the 2013 UNICEF report Canada, Greece and the United States of America were the only countries with a prevalence of childhood overweight/obesity higher than 20%, Portugal was the fourth country on the list2.
Obesity was also identified as a strong and potentially modifiable risk factor for the development and progression of kidney disease3. In children, recent data confirmed a similar trend. In 2013, a study characterizing the European paediatric population under renal replacement therapy revealed that more than 30% of the children were overweight or obese4. This data is particularly concerning since it has been shown that higher BMI is significantly associated with an increased risk of death among children with end‑stage renal disease5.
Pretransplantation obesity and increased BMI after renal transplant were also associated with decreased renal allograft survival in paediatric patients6. Moreover, besides the impact of obesity as a risk factor for disease progression when kidney impairment already exists, two recent cohort studies showed that otherwise healthy overweight and obese children are at a significantly increased risk of all‑cause end‑stage renal disease later in life7,8.
The so‑termed obesity‑related glomerulopathy, a secondary form of focal segmental glomerulosclerosis, morphologically characterised by glomerulomegaly, mesangial cell proliferation and matrix accumulation, was first described in 1975 by Cohen in massive obesity patients with normal renal function. Since then, this histological pattern has been repeatedly found in pathology studies and, in 2001, Kambham et al. reported a tenfold increase in the biopsy incidence of obesity‑related glomerulopathy in a 15‑year period. Obesity‑related glomerulopathy is described as having a lower incidence of nephrotic syndrome and a more indolent course with slower progression of proteinuria and renal failure, milder foot‑process fusion, lesser segmental sclerosis and more glomerulomegaly, compared to idiopathic focal segmental glomerulosclerosis.
Nonetheless, in children, only a few studies have addressed the impact of obesity on the kidney and obesity‑related nephropathy is still a virtually non‑diagnosed entity. The kidney damage is thought to be initiated by an hyperfiltration phase, that initially functions as a physiological adaptation of the kidney to the increased body mass. The chronic state of hyperfiltration later potentiates progressive renal damage, with increased loss of proteins and a last phase of glomerulomegaly, cellular remodelling and fibrotic scaring.
Renal tubulo‑interstitial fibrosis is a non‑specific process that represents the final common pathway for all kidney diseases. The gradual expansion of fibrotic tissue destroys the normal kidney structure and results in organ dysfunction and is known to be associated with the local release of several biologically active factors.
It is believed that some degree of renal impairment associated with obesity starts early in childhood, long before the appearance of hypertension, diabetes and other associated comorbidities known to contribute to renal disease. Even so, the association of renal injury with obesity is still a debated question, since few studies exist and contradictory results continue to emerge.
]]> Some authors reported strong positive correlations between measures of obesity and GFR, probably reflecting an hyperfiltration state, while others found lower GFR levels in overweight/obese children or no differences.Prevailing evidence suggests that glomerular leaking of albumin is a reflection of general vascular damage. Obesity is associated with endothelial dysfunction and intimae‑media thickness but its association with microalbuminuria or overt proteinuria during childhood is not well established and is variable among existent studies.
These contradictory findings might result from the fact that it is particularly difficult to evaluate renal function in the general paediatric population and to which extent the kidney is involved in the metabolic cluster of conditions that emerge with the onset of obesity in early ages. Firstly, since it is not justifiable to apply exogenous and more accurate, but invasive, methods in healthy children, one has to rely on estimation GFR formulas or in the 24‑h urine creatinine clearance (CrCl). However, formulas to estimate GFR are known to have some limitations and 24‑h urine samples might be difficult to reliably obtain in children.
Secondly, the degree of kidney involvement related to obesity might be subtle, below the threshold to translate into changes in classic markers. The emergence of cystatin C was expected to overcome some of the limitations of creatinine‑based estimations, adding an improved clinical sensitivity in early renal damage.
Though, studies in adults showed that cystatin C levels are increased in obese subjects and that cystatin C‑based formulas may result in an underestimation of GFR in patients with higher BMI9. Few studies exist on cystatin C levels in children, leaving a large uncertainty regarding the influence of body composition in the interpretation of cystatin C levels.
Several studies in children reported GFR estimation formulas to be reliable methods to assess kidney function but the accuracy of 24‑hour creatinine clearance was rarely reported. It has long been recognized that 24‑hour creatinine clearance can be affected by inaccuracies in the quantity of urine collected and that tubular secretion of creatinine falsely elevates the GFR estimation. In a recent paper of our group, we found that GFR estimation using Zappitelli combined formula (using creatinine and cystatin C values) was the closest to the 24‑hour creatinine clearance10. A recent study in adults addressed the issue of possible differential performances of GFR equations, either including creatinine, cystatin C or both, in subgroups defined by body composition11. The authors reported that, in comparison with exogenous methods for GFR determination, both creatinine‑and cystatin C‑based equations underestimated GFR in people with higher BMI and that the higher absolute differences were found in people with normal renal function. The absolute differences and bias among subgroups were smallest for combined equations and the authors advocated the preferential use of combined formulas. These findings are in line with studies that found a good agreement of Zappitelli combined formula and exogenous GFR determinations and are concordant with the recommendation to prefer combined formulas, especially in subgroups in which body composition might interfere11. The use of creatinine and cystatin C in combination seems to result in improved accuracy, with the effects of the non‑GFR determinants of each marker being more attenuated than when using each one alone.
Moreover, in general, the studies compare exclusively body surface area (BSA) indexed GFR values. Some authors argued that the scaling of GFR to BSA might be misleading, especially in overweight and obese individuals.
In fact, some authors even defend that, in epidemiological studies including overweight and/or obese individuals, where kidney function is an issue, BSA adjustment should be avoided, since it might imply an important underestimation of renal function in subjects with higher BMI12.
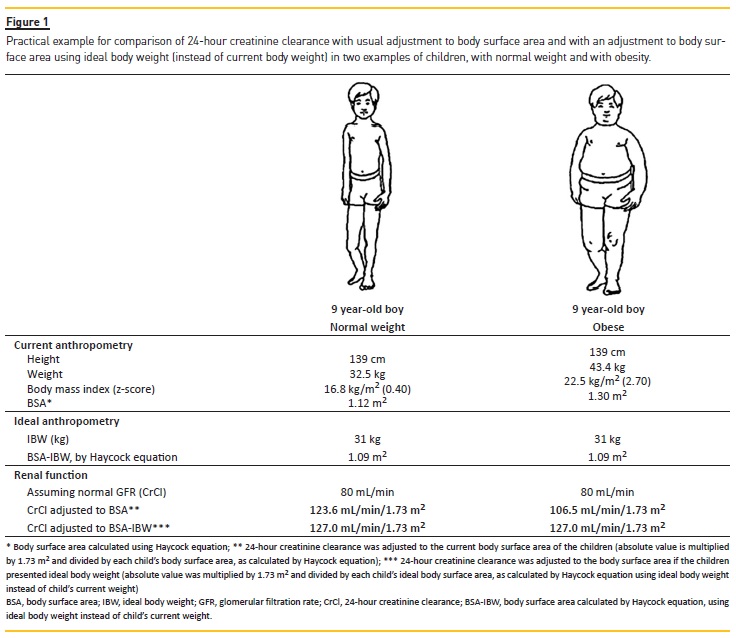
In a recent study of our group, we found that compared to normal weight children, mean absolute GFR (both measured, 24‑hour urine creatinine clearance, and estimated, by several formulas, such as combined Schwartz and combined Zappitelli formulas) was higher in the overweight and obese children, whereas BSA‑adjusted GFR was lower13. In Figure 1, we present a the same height and assuming the same renal function (absolute CrCl = 80 mL/min), but with different body weight that helps to better understand the issue of GFR normalisation in obese individuals. It becomes evident that the normal weight boy has similar values of BSA derived from actual and ideal body weight, thus presenting a minimal difference in the respective adjusted CrCl values. On the other hand, in the obese boy, actual BSA is 1.30 m2 whereas the IBW‑derived BSA equals that of the normal weight boy, resulting in a difference in adjusted CrCl of about 20 mL/min/1.73 m2.
Thus, it becomes evident that these important inconsistencies introduced by GFR adjustment for body size in overweight and obese children result from the fact that normalisation to conventional BSA, a body size descriptor dependent on weight, systematically yields lower GFR estimates in these children than in normal weight children. The finding of an increased absolute GFR in the overweight and obese children is consistent with a state of glomerular hyperfiltration as the initial stage of obesity‑associated renal dysfunction.
]]> Nonetheless, acknowledging that GFR varies with weight and height, GFR must include some adjustment for body size. But the problem that has gained importance with the obesity epidemic of the last few decades is that, although varying with weight and height, the kidney size and the number of functioning nephrons will not increase if an individual of a certain height and weight gains additional fat mass and becomes obese at some point of the life course. So, at any undetermined moment of weight gain, when adjusting for real BSA we will start over adjusting. Thus, we believe that, in addition to trying to evaluate the true impact of obesity in the kidney function in future studies, albeit using exogenous GFR determination methods, it is crucial to consider that the method of adjustment for body size might be a major confounder of GFR determination in individuals with abnormal body habitus. Although some previous studies in adults have addressed this issue14, the non‑negligible differences found in our study are exceedingly important to daily clinical practice and have not been previously explored in the paediatric population.MECHANISMS OF OBESITY‑RELATED KIDNEY INJURY
The possible mechanisms through which obesity might cause renal impairment are diverse and still poorly understood and insufficiently studied, especially in children.
Adipose tissue is involved in the production of several bioactive molecules, such as adiponectin, leptin, inflammatory and oxidative stress molecules, even in children, and the recognition that many of these substances may affect several cellular components in the kidney and cause pathological changes has been an important focus of research. Moreover, it has been speculated that the local production of active fibrotic cytokines, identified as markers of disease activity and histopathological deterioration in several kidney diseases, might also be increased in obesity.
In the same group of 8‑to 9‑year‑old children whose renal function was evaluated, we also tried to address and evaluate some of the mechanisms underlying the association between obesity and kidney injury. The fibrotic process that is initiated in obesity is believed to involve the infiltration of the renal interstitium by immune cells and fibroblasts, followed by a fibrogenic signalling phase in which several cytokines are released from resident renal cells, namely endothelin‑1 and transforming growth factor‑β1 (TGF‑β1).
Since the urinary excretion of these cytokines has been proven to reflect their intrarenal production, both might be used as markers of tissue damage severity and have been reported to be increased in children with a wide spectrum of kidney conditions15. We hypothesized that high levels of urinary cytokines might also be increased in overweight and obese children, reflecting renal haemodynamic changes and some initial degree of inflammation, overactivation of the renin‑angiotensin‑aldosterone system (RAAS) and tissue injury. Whereas our initial hypothesis of higher levels of urinary fibrogenic cytokines in obese children was not confirmed, both TGF‑β1 and endothelin‑1 levels were associated with urinary angiotensinogen levels, which likely reflects an early interplay between tissue remodelling and RAAS in obesity‑related kidney injury. Should this renal RAAS‑cytokine interaction be sustained, it would feed a deleterious pathway, in which normal cytokine‑mediated tissue repair in response to acute injury gives place to progressive fibrosis, ultimately causing kidney impairment. Our results suggest that even in the early phases of kidney injury inflicted by excessive adipose mass, the association between urinary cytokines and intrarenal RAAS already exists, clarifying another pathologic mechanism operating early on obesity‑related kidney injury16.
In fact, the obesity‑RAAS‑hypertension axis is known to be closely related to the development of renal disease, as the increased release of adipose‑tissue derived‑RAAS components into the circulation will affect haemodynamic homeostasis and the intrarenal RAAS itself.
There is substantial evidence that most angiotensin II present in renal tissues is delivered to the kidney from the circulation, but it is also generated locally from intrarenal angiotensinogen, produced by the proximal tubule cells. Directly and indirectly, angiotensin II can enhance capillary filtration pressure and promote proteinuria, essentially by nephrin dephosphorylation during podocyte apoptosis and by decreasing proteoglycans production, thus impairing filtration of high molecular weight proteins. Besides helping to maintain blood volume and blood pressure stability, angiotensin II can also function as a multifunctional cytokine, with an important role in cell proliferation, hypertrophy, reactive oxygen species production, inflammation and extracellular matrix deposition.
Both insulin and leptin are also thought to contribute to renal injury and to the progression of chronic kidney disease by several mechanisms. Insulin has several effects in different parts of the nephron. At the tubular level, insulin has an antinatriuretic effect and increases sodium reabsorption. The effects at the glomerular level are somehow contradictory; in experimental studies insulin was shown to increase GFR possibly due to its vasodilator effect, but studies in humans found the opposite or no effect on GFR. Insulin resistance is believed to reduce noradrenaline‑induced efferent arteriolar constriction, raising the transcapillary pressure gradient and hydrostatic pressure and causing hyperfiltration.
Furthermore, insulin can modulate the production or action of other growth factors, such as TGF‑β1 and ET‑1, and points of interaction with the RAAS have been described. Leptin is known to stimulate the sympathetic nervous system, promoting sodium reabsorption by the kidney and increasing blood pressure. It can also induce inflammatory activity, by increasing the production of several inflammatory cytokines, reactive oxygen species and monocyte proliferation. Adiponectin and others more recently discovered adipokines, such as resistin and visfatin, are also believed to play a role in the kidney dysfunction process but scarce evidence exists so far. Oxidative stress represents another important mechanism underlying progression of renal injury in obesity, since reactive oxygen species can cause direct cell injury, promoting glomerular and tubule injury and proteinuria. Moreover, reactive oxygen species and inflammatory molecules contribute to progressive vascular dysfunction, impaired endothelium‑dependent vasodilatation and activation of adhesion molecules, which can also indirectly affect the kidney by interfering with its vasculature and haemodynamics.
]]> In brief, obesity is a well‑recognized low‑grade inflammatory and pro‑oxidant state which, along with an overactivated RAAS, might be among the underlying mechanisms determining the association between obesity and altered metabolic states, vascular dysfunction and kidney impairment.Overall, in this editorial we present substantial evidence on the impact of obesity on the young kidney.
The recognition of obesity, as a major detrimental determinant for cardiovascular health and renal function in young children, should make clinicians aware of the importance of implementing early strategies to prevent and fight childhood obesity.
References
1. Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980‑2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014; 384:76681. [ Links ]
2. Adamson P. Child Well‑being in Rich Countries: A comparative overview. Papers, vol. 683, Innocenti Report Card; 2013, p. 158. [ Links ]
3. Hsu C, McCulloch CE, Iribarren C, Darbinian J, Go AS. Body mass index and risk for end‑stage renal disease. Ann Intern Med. 2006; 144:218. [ Links ]
4. Bonthuis M, van Stralen KJ, Verrina E, et al. Underweight, overweight and obesity in paediatric dialysis and renal transplant patients. Nephrol Dial Transpl. 2013;28(Suppl 4):iv195iv204. [ Links ]
5. Wong CS, Gipson DS, Gillen DL, et al. Anthropometric measures and risk of death in children with end‑stage renal disease. Am J Kidney Dis. 2000; 36:8119. [ Links ]
6. Mitsnefes MM, Khoury P, McEnery PT. Body mass index and allograft function in pediatric renal transplantation. Pediatr Nephrol. 2002; 17:5359. [ Links ]
7. Vivante A, Golan E, Tzur D, et al. Body mass index in 1.2 million adolescents and risk for end‑stage renal disease. Arch Intern Med. 2012; 172:164450. [ Links ]
8. Silverwood RJ, Pierce M, Hardy R, et al. Early‑life overweight trajectory and CKD in the 1946 British birth cohort study. Am J Kidney Dis. 2013; 62:27684. [ Links ]
9. Vupputuri S, Fox CS, Coresh J, Woodward M, Muntner P. Differential estimation of CKD using creatinine‑versus cystatin C‑based estimating equations by category of body mass index. Am J Kidney Dis. 2009; 53:9931001. [ Links ]
10. Correia‑Costa L, Afonso AC, Schaefer F, et al. Decreased renal function in overweight and obese prepubertal children. Pediatr Res. 2015; 78:43644. [ Links ]
11. Fan L, Inker LA, Rossert J, et al. Glomerular filtration rate estimation using cystatin C alone or combined with creatinine as a confirmatory test. Nephrol Dial Transpl. 2014; 29:1195203. [ Links ]
12. Wuerzner G, Bochud M, Giusti V, Burnier M. Measurement of glomerular filtration rate in obese patients: pitfalls and potential consequences on drug therapy. Obes Facts. 2011; 4:23843. [ Links ]
13. Correia‑Costa L, Schaefer F, Afonso AC, et al. Normalization of glomerular filtration rate in obese children. Pediatr Nephrol. 2016 (accepted for publication). [ Links ]
14. Delanaye P, Krzesinski J‑M. Indexing of renal function parameters by body surface area: intelligence or folly? Nephron Clin Pr. 2011; 119:c28992. [ Links ]
15. Grenda R, Wühl E, Litwin M, et al. Urinary excretion of endothelin‑1 (ET‑1), transforming growth factor‑beta1 (TGF‑beta1) and vascular endothelial growth factor (VEGF165) in paediatric chronic kidney diseases: results of the ESCAPE trial. Nephrol Dial Transpl. 2007; 22:348794. [ Links ]
16. Correia‑Costa L, Morato M, Sousa T, et al. Urinary fibrogenic cytokines ET‑1 and TGF‑β1 are associated with urinary angiotensinogen levels in obese children. Pediatr Nephrol. 2016; 31:45564. [ Links ]
Liane Correia‑Costa,
]]> M.D., PhDEPIUnit Institute of Public Health, University of Porto, Porto, Portugal
Rua das Taipas nº 135, 4050‑600
Porto, Portugal
Phone: +351 222 061 820
Fax: +351 222 061 821
Email: liane@med.up.pt
Disclosure of potential conflicts of interest: None declared
]]> Received for publication: May 15, 2016
Accepted in revised form: Jun 3, 2016
]]>{kind=link}