Acute kidney injury due to Q fever
Ana R. Fernandes1, Francisco Gouveia2, Márcio S. R. Viegas1, Sofia S. Coelho1, Elsa Q. Soares1, Nuno Luís3, Ana S. Natário1, José C. Barreto1
1 Nephrology Department, Centro Hospitalar de Setúbal
2 Department of Internal Medicine, Centro Hospitalar Barreiro Montijo
3 Infectious Disease Department, Centro Hospitalar de Setúbal
]]>
ABSTRACT
Coxiella burnetii (C. burnetii) causes a zoonotic disease Q fever. This bacterium is highly resistant to harsh environmental conditions and causes an uncharacteristic clinical syndrome. Q fever may be acute or chronic and renal manifestations of the disease are more common in the chronic forms. It is reported a case of a 83 -year old woman, with previous normal renal function and a medical history of arterial hypertension and osteoarthritis.
She presented with leg oedema, acute kidney injury (serum creatinine 4.14 mg/dl), and an urine protein-to-creatinine ratio of 9.14 gr/gr. A diagnosis of acute kidney injury with nephrotic syndrome was admitted. The lab work revealed a decrease in serum complement levels (C3, C4), and elevated serum levels of β2 -microglobulin and IgM anticardiolipin. Renal ultrasound showed bilateral cysts, so a renal biopsy could not be performed. During hospital stay, renal function worsened with oliguria and the patient needed transient haemodialysis. The renal function gradually recovered but the nephrotic syndrome (ratio 18gr/gr) persisted, with a thrombotic complication (deep vein thrombosis and pulmonary emboli). She presented a fever of unknown origin (FUO) and was treated with several antibiotic courses, eventually becoming afebrile. She was discharged with a serum creatinine 0,89mg/dL and a proteinuria of 18g/24H. By then, we had obtained the result of a positive serology for C. burnetii, so doxycycline was started and proteinuria (0,3gr/gr) remitted. Currently, the patient remains with high levels of C. burnetii antibodies and is still under treatment with doxycycline.
The authors report a case of acute Q fever manifested by recurrent fever and acute kidney injury with nephrotic syndrome. This case illustrates a rare aetiology of nephrotic syndrome with acute kidney injury.
Keywords: Coxiella burnetii infection, membranoproliferative glomerulonephritis, acute kidney injury, nephrotic Syndrome
INTRODUCTION
Q fever is a widespread zoonotic disease caused by the pathogen C. burnetii1.
This bacterium forms spores during intracellular proliferation, becoming resistant to several antimicrobial agents. They are able to change the lipopolysaccharide composition of the membrane during replication, producing antigenic variants (important to the diagnosis)2.
]]> The bacterium is excreted in urine, milk, faeces, and birth products. These products, especially the latter, contain large numbers of bacteria that become aerosolized after drying. Only a small number or C. burnetii organisms are required to cause disease and infection can be acquired via inhalation or skin contact. Direct exposure to a host is not necessary for infection2.The infective potential capacity of the organism, associated to its ability to survive harsh environments3, makes possible the diagnosis of Q fever without a relevant epidemiological context. C. burnetii infected persons may persist asymptomatic through life. However, pregnancy, heart valve disease, prosthetic material, haemodialysis4 or acquired immunodeficiency syndrome (AIDS) may reactivate infection5.Coxiella burnetii infection has both acute and chronic forms and debuts with a wide spectrum of disease manifestations.(6) Glomerular kidney disease is extremely rare and referred to in only a few case reports Chronic forms of disease can be insidious7 and have a protracted course, developing until at most 6 months after infection and occur in approximately 5%8 of the patients.
Review articles of Q fever briefly mention renal dysfunction associated with endocarditis due to chronic infection and do not refer acute renal complications.9 The incidence of renal complications is unknown. Proteinuria is the most common manifestation of renal involvement and glomerular lesions found in biopsies were classified as focal and segmental proliferative, mesangiocapillary or diffuse proliferative glomerulonephritis.10 C. burnetii does not grow in routine blood cultures, so diagnosis must be made based on the results of specific testing. Most cases are diagnosed based on detection of phase I and II antibodies11 (between acute and convalescent paired sera); a 4-fold rise in complementfixing antibody titre against phase II antigen has the highest specificity. This requires a baseline sample and another sample after 3-4 weeks. Serological tests are not helpful in the acute phase of disease but may later confirm the diagnosis: seroconversion generally occurs between days 7 and 15 and is almost always present at 21 days after disease onset.2
The authors report a case of acute Q fever manifested by exanthema, recurrent fever and acute kidney injury with nephrotic syndrome.
CASE REPORT
The authors report a case of an 83-year-old female, with a medical history of arterial hypertension, mitral valve calcification, hyperuricaemia, diverticulosis, hiatal hernia, osteoarthritis and implantation of a total knee arthroplasty several years prior to admission to hospital due to a 2-month history of leg oedema. Before admission she was prescribed a non-steroidal anti-inflammatory drug (NSAID), due to knee pain related to osteoarthritis. As the symptoms worsened, she noted a reduction in her urine output and came to the hospital.On physical examination her legs and were swollen and patient presented blood pressure of 126/87mmHg and body temperature of 36.3°C. Laboratory tests revealed haemoglobin 11.2 g/dl, with a mean corpuscular volume 90fl and mean corpuscular haemoglobin 30%, normal white cell count, aspartate aminotransferase 25 UI/L, alanine aminotransferase 19 UI/L, urea 138 mg/dL, creatinine 4.14 mg/dl (previous creatinine was 1 mg/dl); sodium 132.0 mEq/l, potassium 5.9 mEq/l; C reactive protein (CRP) 5.50 mg/dl. Thyroid function was normal. Albumin was 1.3 g/dl and total cholesterol 186 mg/dl.
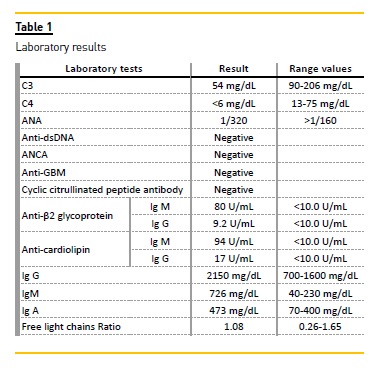
Urinalysis revealed proteins +++ and an urine protein-to-creatinine ratio of 9.14 gr/gr. Antinuclear antibodies were positive with a titre of 1/320 with speckled pattern, anti -double -strand DNA, anti-neutrophil cytoplasmic antibody and anti -glomerular basement membrane antibody were negative. C3 was 54 mg/dl and C4 < 6 mg/dl. β2 -microglobulin IgM was 80 U/ml and anticardiolipine IgM 94 U/ml. Measurement of IgG 2150 mg/dl, IgM 726 mg/dl, IgA 473 mg/dl. (Table 1) Protein electrophoresis showed an oligoclonal peak in the gama fraction. Serum immunofixation showed polyclonal gammopathy IgM lambda and IgG kappa, interpreted as secondary to inflammatory disease.
Serology for viral hepatitis B and C, human immunodeficiency virus and syphilis were negative. Chest x -ray was unremarkable.
]]> Renal ultrasound showed kidneys within normal size with regular contours, diminished corticomedullary differentiation and numerous cortical and parapyelic cysts bilaterally, the largest 8 cm in diameter. Doppler ultrasound excluded renal vessel thrombosis.Transthoracic echocardiogram revealed hypertrophy of the left ventricle, without valvular disease.
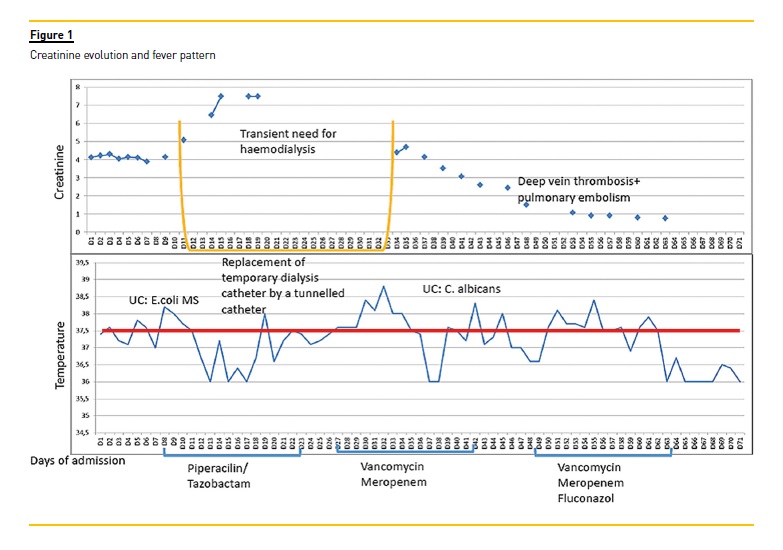
Subsequently, the patient developed oliguria; renal function deteriorated (creatinine 5,26 mg/dl) and the patient started haemodialysis on the 11th day of admission. (Figure 1)
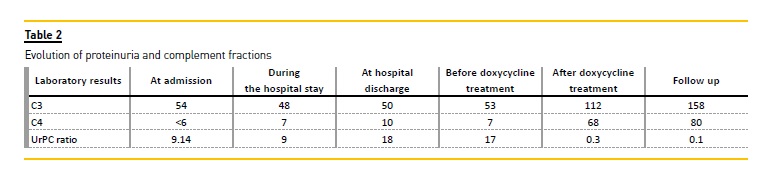
Based on the diagnosis of nephrotic syndrome in a patient with hypocomplementaemia and no evident underlying cause, we admitted a primary membranoproliferative glomerulonephritis. On the 7th day of admission, the patient had fever and a rise in CRP and urinalysis was suggestive of urinary tract infection, so she was started on piperacillin/tazobactam. E. coli was isolated in urine. After 15 days of antibiotics, the patient continued to show intermittent fever. The haemodialysis catheter was replaced by a tunneled catheter and there was another rise in inflammatory parameters accompanied by fever, so blood cultures were drawn and vancomycin started, and the catheter removed, assuming a central line-associated bloodstream infection. Blood cultures were sterile and transoesophageal echocardiogram excluded vegetations. As fever persisted, meropenem and fluconazole were added to vancomycin and this treatment was maintained for 12 days. Urine output gradually increased with improvement of renal function and dialysis was suspended, though proteinuria remained high (18g/24h). (Table 2)
Inflammatory parameters started to decrease and fever resolved. At this point, patient presented with asymmetrical leg oedema, and echodoppler of the lower limb showed thrombosis of the left femoral and popliteal veins.
The thoracic computed tomography angiography showed a cloth in the right pulmonary artery. We suspected an embolic phenomenon related to the nephrotic syndrome and treatment with low molecular weight heparin was started. The patient was discharged with a creatinine 0,89mg/dl after remaining afebrile for one week. Serology for C. burnetii, available at the time of discharge, showed phase II IgG 1/400 and IgM >200. We diagnosed Q fever and the patient was treated with doxycycline 100 mg bid for 2 weeks. After making this diagnosis, we carefully asked again for any risk factor for this infection and the patient continued to deny any epidemiological context. The patient was evaluated one month after discharge and an improvement in renal function was seen, with creatinine 0.9mg/dL and the urine protein -to -creatinine ratio 0.3 gr/gr. Antiphospholipid antibodies were negative. She was referred for evaluation by an Infectious diseases specialist. C. burnetii antibody titres remained positive 12 months after the acute onset of the disease (phase II IgG 1/400 and an IgM 200), so doxycycline treatment was started assuming a chronic infection.
DISCUSSION
In humans, acute C. burnetii infection is often asymptomatic or mistaken for an influenza -like illness or atypical pneumonia. The predominant form of acute Q fever is self -limited febrile illness2.
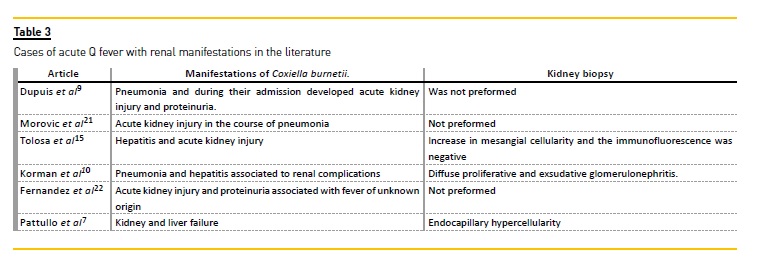
We presented a case of nephrotic syndrome, associated with fever and acute kidney injury. The main manifestation of acute Q fever in this patient was glomerulonephritis presenting as nephrotic syndrome. Proteinuria is the main manifestations of kidney disease in acute Q fever12.Revision of incipient current literature (Table 3) shows that the causes associated with acute kidney injury in Q fever could be acute tubular necrosis, rhabdomyolysis, proliferative GN, tubulointerstitial nephritis.
The pathogenesis of Q fever, in particular acute infection, is poorly understood, because of the selflimiting nature of the illness and low mortality rates13. Examination of biopsy specimens obtained during acute C. burnetii infection shows a major inflammatory response but few organisms14. The three renal biopsies described in the literature revealed cellular proliferation7,10,15. Our patient had a decrease in complement levels, which was consistent with the immune complex deposition characteristic of infectious glomerulonephritis. The histological pattern most often associated with these diseases is the membranoproliferative pattern. Because of this the authors think that if they could have performed a renal biopsy, this would have been the pattern they would find. We associate this nephrotic syndrome to the C. burnetii infection because of the remission of the clinical features of renal disease after the treatment with doxycycline.
]]> Here we describe the second case of Q fever with acute kidney injury with a transiently need for dialysis.This transient need for renal replacement therapy might be explained by an acute tubular necrosis due to the nephrotic syndrome or to an acute interstitial nephritis caused by the NSAIDs the patient took before admission. In the ATN hypothesis, the immunological glomerular lesion caused by C. burnetii culminated in nephrotic syndrome. Consequently, interstitial oedema resulted in acute tubular necrosis which remitted after gradual fluid removal in dialysis. On the other hand, if the need of dialysis was caused by the AIN, renal recovery is due to the discontinuation of the drug and clearance of the cell infiltrate in the interstitium.
Renal biopsy would have been essential to understand the kind of glomerulonephritis the patient developed, the reason she needed temporary dialysis.
In this case, the patient presented with acute kidney injury associated to nephrotic proteinuria with low complement levels and antiphospholipid antibodies. While we were investigating these features, the patient presented a FUO. The investigation of FUO must be broad and excluding a bacterial infection is essential. Many bacterial infections demonstrate antiphospholipid antibodies. Q fever is associated with a high frequency of anticardiolipin antibody positivity and when patients present only with fever, an estimation of these antibodies may assist the diagnosis16.
However since both titres were IgM (of IgM antibody) and our patient was 83-years old without any thrombotic event to date, we associate these titres with the infection, and the thrombotic events were probably related to the procoagulant state associated with the nephrotic syndrome.
Acute Q fever is most often a mild disease that resolves spontaneously within 2 weeks17. Doxycycline at 100 mg twice daily for 14 days is the current recommended regimen for acute Q fever. Because of the risk of chronic infection, clinical and serologic follow-up for 2 years is recommended, particularly in individuals at risk. Patients with an IgG phase I >1:512 twelve months after treatment should undergo closer serological and clinical follow-up as they may have the highest risk to progress to chronic Q fever18. In this patient, the presence of a knee prosthesis is a condition that predisposes to the development of a chronic form of the disease. Moreover the remaining high titres of phase ÎI Ig G twelve months after the diagnosis led us to think that the patient might be developing a chronic form of the disease. The optimum duration of antibiotic therapy cannot be accurately determined because no definite criteria for C. burnetii cure are currently available. Suggestions have ranged from 1 year of antibiotic therapy19 to indefinite administration of antibiotics20.
An epidemiological link to the transmission of the infection is lacking, but due to long environmental persistence and infective power of the bacteria, this is not uncommon.
CONCLUSION
The true prevalence of C. burnetii is underestimated due to scant epidemiological data, lack of accurate diagnostic tests and atypical manifestations of the disease, making this diagnosis easily pass unnoticed. This case illustrates a rare aetiology of nephrotic syndrome with acute kidney injury.
]]> References
1. Honarmand H. Q Fever: An old but still a poorly understood disease. Interdisciplinary Perspectives on Infectious Diseases. 2012:131932 [ Links ]
2. Santos AS, Bacellar F, França A. Febre Q: revisão de conceitos. Revista Medicina Interna. 2007;14:90-99 [ Links ]
3. Arricau -Bouvery N, Rodolakis A. Is Q fever an emerging or re -emerging zoonosis? Veterinary Research. 2005;36:327-349 [ Links ]
4. Dupont HT, Thirion X, Raoult D. Q fever serology: cutoff determination for microimmunofluorescence. Clin Diagn Lab Immunol. 1994;1:189-196 [ Links ]
5. Raoult D, Brouqui P, Marchou B, Gastaut JA. Acute and chronic Q fever in patients with cancer. Clin Infect Dis. 1992;14:127-130 [ Links ]
6. Parker NR, Barralet JH, Bell AM: Q fever. Lancet. 2006;367:679-688 [ Links ]
7. Pattullo Guindi M, Herzenberg A, Scholey J, Wong F. Unexpected renal and liver failure. Am J Med. 2010;123:799-801 [ Links ]
8. Center for Disease Control and prevention. Symptoms, diagnosis, and treatment of Q fever, http://www.cdc.gov/qfever/symptoms/index.html [ Links ]
9. Tissot -Dupont H, Raoult D. Q fever. Infect Dis Clin North Am. 2008;22:505-514 [ Links ]
10. Korman TM, Spelman DW, Perry GJ, Dowling JP. Acute glomerulonephritis associated with acute Q fever: case report and review of the renal complications of Coxiella burnetii infection. Clin Infect Dis. 1998;26:359-64 [ Links ]
11. Million M, Raoult D. Recent advances in the study of Q fever epidemiology, diagnosis and management. J Infect. 2015;71(1):S2-S9 [ Links ]
12. Dupuis G, Peter O, Pedroni D, Petite J. Aspectes cliniques observés lors d'une epidemie de 415 cas de fièvre Q. Schweiz Med Wochenschr. 1985;115:814-818. [ Links ]
13. Spelman DW. Q fever: a study of 111 consecutive cases. Med J Aust 1982; 1:547-53 [ Links ]
14. Reimer LG. Q fever. Clin Microbiol Rev. 1993;6:193-198 [ Links ]
15. Raoult D, Marrie T. Q fever. Clin Infect Dis. 1995;20:489-496 [ Links ]
16. Tolosa -Vilella C, Rodrıguez -Jornet A, Font-Rocabanyera J, Andreu -Navarro X. Mesangioproliferative glomerulonephritis and antibodies to phospholipids in a patient with acute Q fever: case report. Clin Infect Dis. 1995;21:196-198 [ Links ]
17. Asherson R, Cervera R. Antiphospholipid antibodies and infections. Ann Rheum Dis. 2003;62:388-393 [ Links ]
18. Maurin M, Rao D. Q fever. Clin Microbiol Rev. 1999;12(4):518-553 [ Links ]
19. Wielders CC, van Loenhout JA, Morroy G, et al. Long -term serological follow -up of acute q-fever patients after a large epidemic. PLoS ONE 10(7): e0131848. doi:10.1371/journal. pone.0131848 Wilson HG, Neilson GH, Galea EG, Stafford G, OBrien MF. Q fever endocarditis in Queensland. Circulation. 1976;53:680-684 [ Links ]
20. Pedoe HD. Apparent recurrence of Q fever endocarditis following homograft replacement of aortic valve. Br Heart J. 1970;32:568-570 [ Links ]
21. Morovic M, Dzelalija B, Novakovic S, Stankovic S, Dujella J. Acute renal failure as the main complication of acute infection with Coxiella burnetii [letter]. Nephron. 1993;64:335 [ Links ]
22. Fernández S, Pérez VR. Insuficiencia renal como complicación de la fiebre Q aguda [letter]. Med Clin (Barc). 2003;120(15):597-599 [ Links ]
Ana R. Fernandes
Nephrology Department
Centro Hospitalar de Setúbal Setúbal, Portugal
E-mail: anar.fernandes@sapo.pt
]]>Diclosure of conficts of interest: none declared
Received for publication: Jun 9, 2016
Accepted in revised form: Nov 3, 2016
]]>{kind=link}
{kind=link}
{kind=link}