IgA nephropathy in a young adult with nephrotic
syndrome: Case report
João Cassis1, Henrique Silva Sousa2, Rita Theias Manso3, Sância Ramos1, Domingos Machado4
1 Pathology Department, Centro Hospitalar de Lisboa Ocidental, Lisbon Portugal.
2 Nephrology Department, Hospital das Forças Armadas, Lisbon Portugal.
3 Pathology Department, Hospital Dr. Fernando Fonseca, Lisbon Portugal.
4 Nephrology Department, Centro Hospitalar de Lisboa Ocidental, Lisbon Portugal.
]]>
ABSTRACT
IgA nephropathy has many clinical presentations, of which nephrotic syndrome is possibly the rarest. Recently, the association of IgA nephropathy with minimal change disease was better described with patients having complete response to steroid therapy and no progression to CKD. We report a similar case in a young male presenting with nephrotic syndrome.
Keywords: IGA nephropathy, minimal change disease, nephrotic syndrome.
INTRODUCTION
IgA nephropathy (IgAN) is the most common cause of primary glomerulonephritis (GN) worldwide and a major cause of CKD and renal failure. Clinical presentation is varied but asymptomatic haematuria with progressive kidney disease is the most frequent manifestation1.
Nephrotic syndrome is rare but has long been associated with IgAN2. Although proteinuria is as an independent predictor of unfavorable renal outcome3, patients with nephrotic syndrome in IgA seem to have a different outcome. Recent evidence have shown that mild IgAN (M0/1 E0 S0 T0 C0 Oxford Classification) with diffuse foot process effacement on electron microscopy (EM) corresponds to IgAN with superimposed minimal change disease (MCD) and that these patients have remarkably good prognosis with steroid therapy4,5. We hereby report a case of IgAN presenting with nephrotic syndrome.
]]> CASE REPORT19‑year‑old male, complaining of strep throat, prescribed Clarithromycin. Two days later he developed generalized oedema. After one week he presented to the ER with hypertension (141/98mmHg) and anasarca. No signs of inflamed throat. Chest XR showed bilateral pleural effusion. Laboratory tests showed haemoglobin levels of 15.2g/dl, 8000 leucocytes count and 214000 platelets.
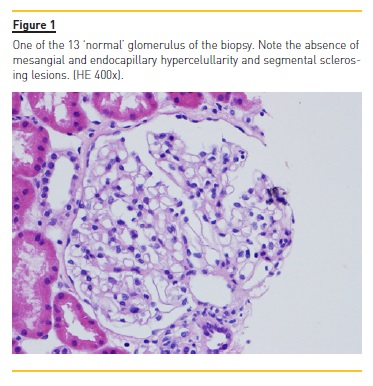
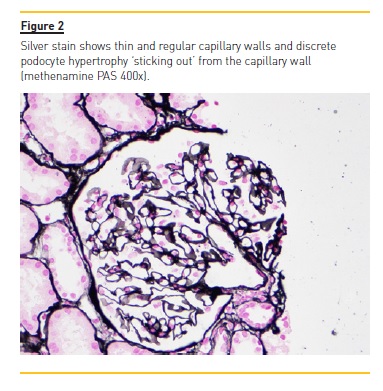
Serum creatinine was 0.84mg/dl with eGFR 127ml/min/m2; with hypoproteinaemia (3,8g/dl); and hypoalbuminaemia (1.9g/dl); total cholesterol 419mg/dl; LDL 327mg/dl. Liver function, serum protein electrophoresis, and complement were normal; ANAs, ANCAs, ASOT and viral serologies negatives. Urine dipstick with proteinuria 4+, haematuria 1+; urinary protein/creatinine ratio was 9267mg/g and urinary albumin/creatinine ratio 8442mg/g. A renal biopsy was performed. A total of 13 glomeruli were observed, all normal in size, showing mild podocyte hypertrophy, but otherwise unremarkable (Figure 1 and 2). Tubular epithelium had protein reabsorption droplets.
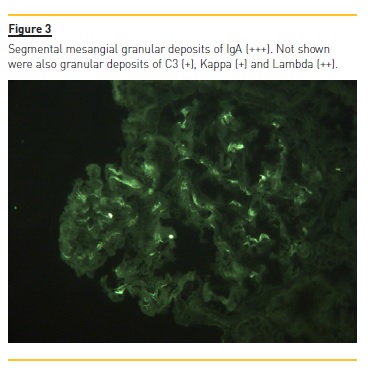
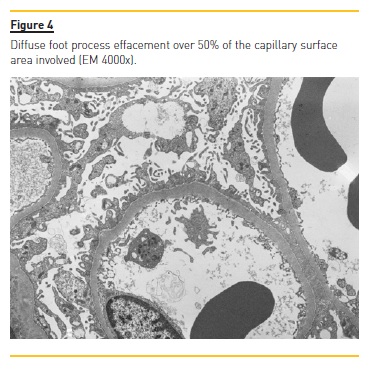
Interstitium and vessels were normal. Immunofluorescence showed granular mesangial IgA deposits (++) (Figure 3), C3 (+), Kappa (+) and Lambda (++). Electron microscopy showed mesangial deposits and diffuse foot process effacement (Figure 4). A IgAN (M0 E0 S0 T0 C0) was diagnosed with superimposed minimal change disease.
]]> Prednisone (60mg q.d.) was started with fairly fast response, decreasing proteinuria, and normalization of serum albumin and cholesterol levels. Patient was lost to follow‑up 2 months after biopsy.
DISCUSSION
IgAN presentation with nephrotic syndrome is rare and usually associated to endocapillary proliferation, segmental sclerosis, and crescent formation (Oxford classification: M1 E1 S1 T1/2 C1/2). On the other hand, patients with Nephrotic Syndrome associated with mild IgAN (M0/1 E0 S0 T0 C0) seem to have a better prognosis4.
According to Herlitz et al, these patients have a dual glomerulopathy with superimposed MCD. A recent cohort established a clear clinical‑pathological difference between IgAN‑MCD and IgA without MCD5. Almost all patients with IgAN‑MCD in this cohort (n=247) had a complete response to steroids and none progressed to ESRD. Although more studies are warranted, it seems to be a growing evidence that proteinuria in itself is not an independent worse prognostic factor. Only electron microscopy (EM) can effectively document diffuse foot process effacement and make the diagnosis of superimposed MCD in these cases. We recommend performing EM on all IgAN cases presenting with nephrotic syndrome and low Oxford classification as these patients have improved prognosis with steroid therapy and extremely unlikely progression to ESRD.
References
1. Rodrigues JC, Haas M, Reich HN. IgA nephropathy. Clinical J Am Soc Nephrol 2017;12(4) 12.4:677‑686 [ Links ]
2. Barbiano di Belgiojoso G, et al. Steroid‑sensitive nephrotic Syndrome with mesangial IgA deposits: a separate entity? Am J Nephrology 1986;6(2):141‑145 [ Links ]
3. Le, WeiBo et al. Long‑term renal survival and related risk factors in patients with IgA nephropathy: results from a cohort of 1155 cases in a Chinese adult population. Nephrol Dial Transpl 2012;27(4):1479‑1485 [ Links ]
4. Herlitz, Leal C, et al. IgA nephropathy with minimal change disease. Clin J Am Soc Nephrol 2014; CJN‑11951113 [ Links ]
5. Li, Xiao‑Wei, et al. Long‑term outcome of IgA nephropathy with minimal change disease: a comparison between patients with and without minimal change disease. Nephrology 2016;29(4):567‑573 [ Links ]
João Cassis
Pathology Department, Centro Hospitalar de Lisboa Ocidental, Lisbon Portugal
E-mail: joaopcassis@gmail.com
Disclosure of potential conflicts of interest: none declared
Received for publication: Jun 11, 2017
]]> Accepted in revised form: Jun 19, 2017 ]]>