Tell me your weight before kidney transplant and Ill tell you your risks
Joana Silva Costa1, Emanuel Ferreira1, Rita Leal1, Catarina Romãozinho1,2, Lídia Santos1, Fernando Macário1,2, Rui Alves1,2, Arnaldo Figueiredo3
1Nephrology Department, Coimbra Hospital and University Center, Coimbra, Portugal 2University Clinic of Nephrology, Faculty of Medicine, University of Coimbra, Portugal 3 Urology and Kidney Transplantation Department, Coimbra Hospital and University Center, Coimbra, Portugal
ABSTRACT
Introduction and aims: Overweight is highly prevalent in kidney transplant candidates and it has been associated with multiple post-transplant complications. In this study, we evaluated the occurrence of complications in the first year after kidney transplantation according to the pre-transplant Body Mass Index of the recipients. Material and methods: Retrospective analysis of patients with age >18 years who underwent first kidney transplantation, between 1st January 2012 and 31st December 2015 in our Center. We analyzed 144 patients, with Body Mass Index: <25 kg/m2 in 48 patients (group 1), 2530 Kg/m2 in 41 patients (group 2) and ≥30 kg/m2 in 55 patients (group 3), maximum of 38.3 Kg/m2. Complications in the first year after the transplant (infection, delayed graft function, surgical/urological complications, cardiovascular disease, hematologic disorders, diabetes, acute rejection, neoplasm, glomerular filtration rate and mortality). were compared between the groups. Statistical analysis was conducted using R Statistical Software version 3.2.5. Results: We found differences between the groups in recipient age and pre-transplant diabetes mellitus and in donor gender. The total number of post-transplant complications was higher in the first 3 months, and >50% occurred in group 3. Infections, mostly urinary, were the main complications during the whole study period, particularly in group 3 (p<0.05). Surgical/urological complications (p<0.01) were also significantly higher in this group during the first 3 months. There was a negative correlation between Body Mass Index and Glomerular Filtration Rate at the time of discharge (regression estimate -0.83 adjusted for age, p=0.018), but not at 1 year post-transplant (regression estimate 0.02, p=0.960). This study highlights the importance of controlling weight before kidney transplantation as obesity is a risk factor for early posttransplant complications, particularly urinary infections and surgical/urological complications.
]]> Key Words: kidney transplantation, obesity, outcomes
INTRODUCTION
Obesity is nowadays recognized as a major global public health problem. This global nature of the obesity epidemic was formally recognized by the World Health Organization (WHO) Expert Consultation on Obesity in 19971. More than one in two adults are overweight or obese in Organisation for Economic Co-operation and Development (OECD) countries and, according to the 2017 Obesity Update, obesity rates are expected to increase further by 2030, affecting not only the developed world but also countries in intermediate development2,3.
The United States, Mexico, New Zealand and Hungary have the higher obesity rates, the first with a rate of 38.2% in 2015. Portugal presented an obesity rate of 16.6% in 2015, lower than the mean OECD rate (19.5%)3. However, obesity prevalence has been increasing in Portugal over the last forty years in both children and adult population, and Body Mass Index (BMI) is ≥25 kg/m2 in more than 50% of the adult population and in more than 80% of the population aged 65 years-old or older4. Obesity has been associated with a higher risk of diabetes, cardiovascular disease, end stage renal disease (ESRD), and consequently with a higher mortality rate in the general population, but also, paradoxically, with a lower risk of mortality in dialysis patients5. There is a survival benefit in ESRD patients who undergo a kidney transplantation (KT) but some studies reported that it is lower in obese (particularly when BMI is ≥40 kg/m2) than non-obese patients5,6. This might be related to an increased risk of infections, delayed graft function (DGF), prolonged surgical times, wound complications, longer hospital admissions and readmission.
However, recent multicenter studies showed that there is still a survival benefit when overweight or obese patients receive a kidney transplant, compared with patients with the same BMI, on the waiting list for KT7.
In this study, our objective was to compare the occurrence of complications in the first year after KT, according to the recipients pre-transplant BMI (<25 Kg/m2, 2530 Kg/m2 and ≥30 kg/m2), in order to identify the main post-transplant complications in the first year and to prepare and inform candidates, pre-transplant, of the post-transplant risks.
MATERIAL AND METHODS
Study Population
Included in the study were patients older than 18 yearsold, who underwent first KT (live or deceased-donor), between 1st January 2012 and 31st December 2015, in our Center. Height and weight measurements were recorded on the day of the transplant and were used to calculate patients BMI. Patients were divided into 3 groups, according to the WHO BMI cut-off points made for overweight and obesity: <25.0 Kg/m2 (underweight or normal weight, group 1), 25.0-29.9 Kg/m2 (overweight, group 2) and ≥30.0 kg/m2 (obesity, group 3)1.
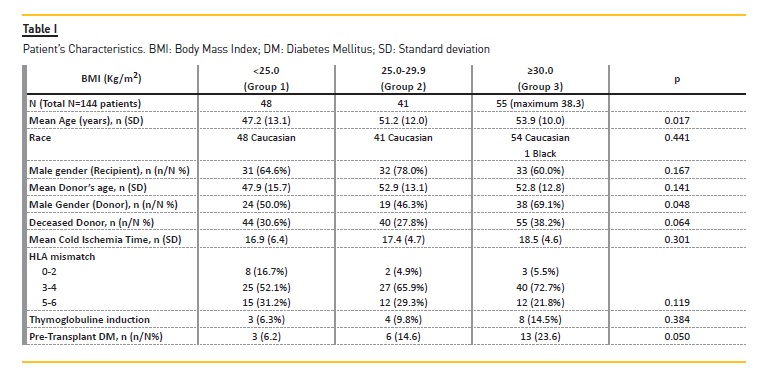
]]> All the recipients with BMI ≥25 Kg/m2 (n=96 patients) were identified and compared with patients with BMI <25 Kg/m2 (n=48 patients). A total of 144 patients, 48 women and 96 men, 143 Caucasian and 1 black, were analyzed. They were divided into 3 groups, according to their BMI: 48 patients with BMI <25 kg/m2 (group 1), 41 patients with BMI 2530 Kg/m2 (group 2) and 55 patients with BMI ≥30 kg/m2 (group 3). Patients maximum BMI was 38.3 Kg/m2.We collected all complications (infection, delayed graft function, surgical/urological complications, cardiovascular disease, hematologic disorders, diabetes, acute rejection, neoplasm, glomerular filtration rate and mortality) in the first year after KT in the patients clinical reports.
Statistical analysis
We conducted a retrospective analysis, comparing the complications in the first year of transplant in patients with BMI <25 Kg/m2, 25-30 Kg/m2 and ≥30 kg/m2. Statistical analysis was conducted using R Statistical Software version 3.2.5.
RESULTS
Obese patients were older (p=0.017) and had more pre-transplant diabetes mellitus (p=0.05). Most of these patients received kidneys from male donors (p=0.048).
No differences were found between the groups in race and gender of the recipients, age of the donor, deceased donor, cold ischemia time, HLA mismatch and thymoglobuline induction (Table I).
The following post-transplant complications results are for the first three months post-transplant, and after that period, for up to one year post-transplant.
Post-transplant results during the first three months
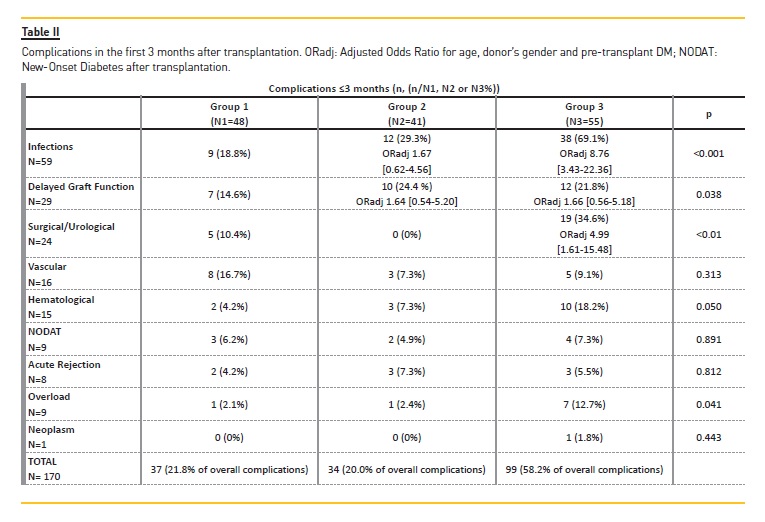
We found more post-transplant complications in the first three months than after that period. Obese patients presented the higher rate of complications during the first three months post-transplant; more than 50% of overall complications (Table II).
]]> The most frequent complications were infections, and they occurred particularly in group 3 (p<0.001), with an adjusted odds ratio 8.76 [3.43-22.36] vs group 1 (adjusted for recipient age, pre-transplant diabetes mellitus and donor gender). Urinary infections were the main type of infection, and more cases were found in group 3. Other observed infections were fever of unknown origin (fever without identified microbiological agents, assumed and treated as infection), respiratory infections, acute gastroenteritis, wound infections and Tenckhoff catheter infections, in descending order of frequency.Delayed graft function, the second main complication, defined as the need for dialysis within the first week post-transplantation, occurred more often in patients with BMI ≥ 25 kg/m2. Of nine patients with overload symptoms (dyspnea and lower limb edema), seven were obese (p=0.041) and four of them also had DGF.
Surgical/urological complications also occurred predominantly in group 3 (p<0.010; adjusted OR 4.99 1.61-15.48]): lymphoceles (4 of 7 lymphoceles occurred in group 3), hematoma around the kidney (4 of 6 hematomas occurred in group 3), urinary fistula (n=4), wound dehiscence (n=3), and obstructive uropathy (n=2). Urinary fistula, wound dehiscence and obstructive uropathy occurred exclusively in patients with BMI≥ 30 kg/m2.
Eleven patients of our study had wound infection or wound dehiscence. The mean age of these patients was 57.5 years (SD 9 years); 9 patients (81.8%) were obese; 2 patients (18.2%) had pre-transplant diabetes, and 2 patients were immunosuppressed with everolimus (18.2%).
No differences between the groups were found regarding vascular complications, New-Onset Diabetes After Transplant (NODAT), acute rejection, hematologic complications or neoplasm. Two patients, one from group 2 and one from group 3, had graft failure associated with vascular complications (arterial and vein thrombosis), in the first few days after KT.
Post-transplant results after the first three months
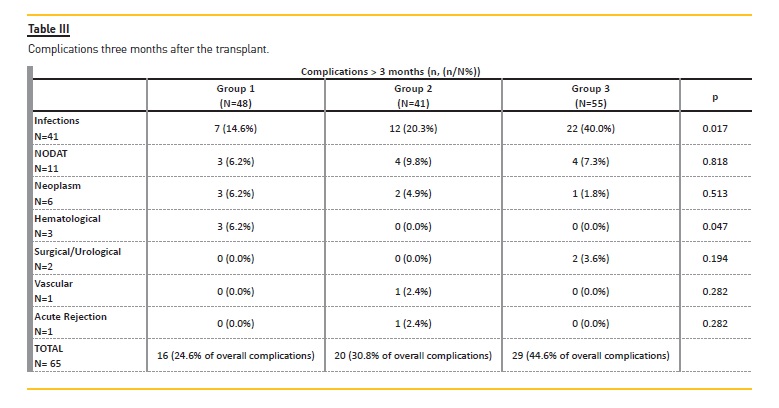
Group 3 also had more post-transplant complications after the first three months, with 44.6% of overall complications (Table III). The main complications were infections (p=0.017, adjusted OR 3.66 [1.36-9.8), particularly urinary (p=0.001). No differences were found between the groups regarding NODAT, neoplasm, surgical/urological and vascular complications or acute rejection.
Glomerular Filtration Rate
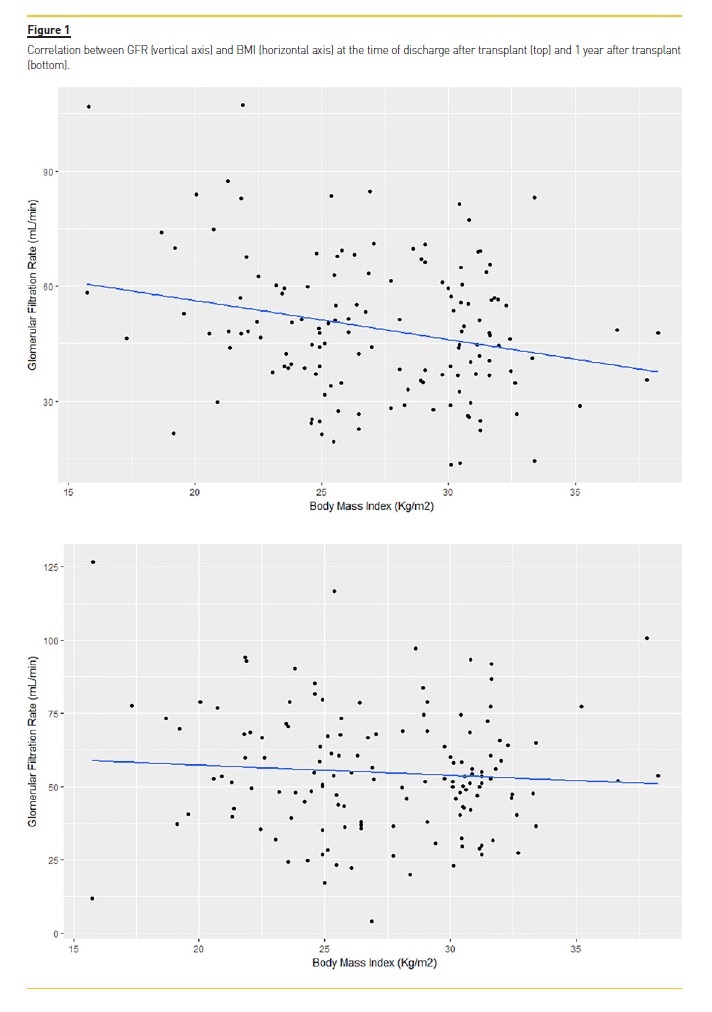
There was a negative correlation between Glomerular Filtration Rate and BMI at the time of discharge after KT (regression estimate -0.83 adjusted for age, p=0.018), but not at 1 year after KT (regression estimate 0.02, p=0.960) (Fig. 1).
Mean hospitalization time
]]> The mean hospitalization time was higher in group 2 (18.17 days, SD 14.32) and the median of each group was 10 days. However, thirty patients had two or more hospitalizations, and half of these patients had BMI ≥30 kg/m2.Mortality
No cases during the study.
Acute coronary Syndrome
No cases during the study.
DISCUSSION
Obesity is an increasing comorbidity among patients with ESRD and its high risk for post-transplant complications requires a cautious pre-transplant evaluation.
We performed this study in order to identify the main complications in the first year of KT, comparing patients grouped by BMI. We found that during this period, patients with BMI≥ 30 kg/m2 presented more complications, particularly in the first three months.
Infections (mostly urinary), DGF and surgical/urological complications (mainly lymphoceles) were the most frequent post-transplant complications in the first three months. Infections and surgical/urological complications occurred particularly in the obese patients, and we found more DGF in patients with BMI ≥25 kg/m2.
There is a well-known predisposition to all types of infections in obese patients (nosocomial, surgical site, odontogenic, respiratory, gastrointestinal, liver and biliary, urogenital, skin, bone and joint infections), particularly after a solid organ or a bone marrow transplant.
]]> That was corroborated by the high rates of posttransplant infections that we found in our study in this group of patients. This predisposition can be due to the proinflammatory state of obesity (release of proinflammatory factors, cytokines, leptin deficiency, among others), but also organ-related factors in obesity.For example, respiratory infections, the third main cause of infections in our study, can also be explained by the higher risk of pulmonary disease in the obese patients (obstructive sleep apnea, with increased risk of aspiration, chronic inflammation of the respiratory tract, dysfunctional respiratory mechanics, among others)8.
DGF is also a frequent complication in obese patients after KT, as high as 40% in recipients with BMI ≥35 kg/m2 according to the literature5,7,9. However, there is no association between DGF and graft survival7,10. In our study we found a negative correlation between Glomerular Filtration Rate and BMI at the time of discharge after KT, but not at one year after KT. Concerning overload symptoms, the association of obesity with congestive heart failure in the peri-transplant period remains a controversial topic5. In our study, we found more cases in the obese patients.
Regarding surgical/urological complications, obesity is a well-known risk factor for lymphoceles, along with diabetes, elderly age of recipient, long time of warm ischemia, acute rejection episodes and delayed graft function11. More cases of wound infections and wound dehiscence were seen in patients with BMI ≥30 kg/m2.
It has been described in the literature that these two complications affect more often obese patients, with an incidence between 4 and 40%, a greater dead space above the fascia, longer operative times and larger incisions being possible explanations5,7,11,12. There are other risk factors for these complications, such as patient age, diabetes, and treatment with mTOR inhibitor drugs, among others5. However, in our study, obesity (81.8% of the patients were obese) was the main risk factor for wound infections and wound dehiscence.
Some studies described an association between obesity and acute rejections. However, in agreement with a recent Systematic Review and Meta-analysis9, we found no association between obesity and acute rejection in our study.
NODAT can occur at any time after KT, but more frequently in the first year, with an incidence of 1525%.
Overweight and obesity are well-known phenotypic risk factors for NODAT. There is a correlation between pre-transplant weight and NODAT, so that the risk of NODAT can increase by 13% for each one-unit increase in BMI13. In our study, we found no differences between the groups for development of NODAT.
In our study, obese patients had no higher hospitalization time, but 50% of the patients who had more than two hospitalizations were obese. Regarding the graft function, we found that obese patients had worse graft function at the time of discharge after transplant, but not at 1 year after the transplant.
According to our study results, controlling the weight before KT may reduce early post-transplant complications, particularly urinary infections and surgical/urological complications.
]]> The main limitations of our study were the low number of patients and the short time of follow-up, which precluded the evaluation of long-term outcomes related to obesity, such as patient and graft survival, cardiovascular events or neoplasm.Another limitation was the use of BMI as the only marker of obesity. Although BMI can be a convenient method to divide patients into categories, some studies have already classified BMI an imperfect metric of body fat mass because it doesnt take into account gender differences of fat mass and doesnt differentiate between adiposity and muscle mass4. The 1997 WHO
Expert Consultation on Obesity recognized the importance of abdominal fat mass (abdominal, central or visceral obesity), and the need to use alternative measures that reflect abdominal adiposity to complement BMI. Waist circumference, waist-hip ratio and waistheight ratio, were proposed by WHO as alternative measures, as they have been suggested as being superior to BMI in predicting cardiovascular disease, the main cause of obesity-related deaths14. Waist circumference seems to be the most practical alternative measure and it should be used in the pre-transplant recipient evaluation, in order to complement BMI.
Finally, since obesity is a potentially modifiable condition, surgeons and nephrologists should encourage patients to lose weight before renal transplantation in order to reduce peri-operative and post-transplant complications. However, obesity is not an absolute contraindication to kidney transplantation (but a relative contraindication in some centers, particularly when BMI ≥40 Kg/m2) and the benefits of transplant in survival and quality of life versus long-term dialysis should also be considered7,15. The access to transplantation in obese patients should be individualized, considering the compliance to the medical recommendations such as reducing their weight, the treatment options such as bariatric surgery, the comorbidities of the patients and their adaptation to dialysis. It is mandatory to inform these patients, during their pre-transplant evaluation, about their risk of worse outcomes after the transplant.
References
1. WHO. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser 2000;894:i-xii,1-253; [ Links ]
2. Caballero, B. The global epidemic of obesity: an overview. Epidemiol Rev 2007;29:1-5; [ Links ]
]]>3. OECD. Obesity Update 2017. Available at https://www.oecd.org/els/health-systems/Obesity-Update-2017.pdf. Accessed December 20, 2017; [ Links ]
4. Camolas J, Gregório MJ, Mendes de Sousa S, Graça P. Obesity: Optimizing the therapeutic approach in the National Health Service. Available at http://www.alimentacaosaudavel.dgs.pt/activeapp/wpcontent/files_mf/1513848603Obesidade_otimizacaodaabordagemterapeuticanoservi%C3%A7onacionaldesaude.pdf. Accessed December 20, 2017; [ Links ]
5. Lesage J, Gill JS. Management of the obese kidney transplant candidate. Transplant Rev 2017;31(1):35-41; [ Links ]
6. Gill, JS, Lan J, Dong J. et al. The survival benefit of kidney transplantation in obese patients. Am J Transplant 2013;13:2083-2090; [ Links ]
7. Liese J, Bottner N, Büttner S, et al. Influence of the recipient body mass index on the outcomes after kidney transplantation. Langenbecks Arch Surg 2018 Feb;403(1):73-82; [ Links ]
]]>8. Falagas ME, Kompoti M. Obesity and infection. Lancet Infect Dis 2006;6(7):438-446; [ Links ]
9. Nicoletto BB, Fonseca NKO, Manfro RC, Gonçalves LFS, Leitão CB, Souza GC. Effects of obesity on Kidney Transplantation Outcomes: a systematic review and meta-analysis. Transplantation 2014;98(2):167-176; [ Links ]
10. Hill CJ, Courtney AE, Cardwell CR, et al. Recipient obesity and outcomes after kidney transplantation: a systematic review and meta-analysis. Nephrol Dial Transplant 2015;30(8):1403-1411; [ Links ]
11. Krajewski W, Piszczek R, Weyde W, Rybak Z, Dembowski J. Lymphocele urological complication after renal transplantation. Postepy Hig Med Dosw (Online) 2013;23(67):326-330; [ Links ]
12. Drafts HH, Anjum MR, Wynn JJ, Mulloy LL, Bowley JN, Humphries AL. The impact of pre-transplant obesity on renal transplant outcomes. Clin Transplant 1997;11:493-496; [ Links ]
]]>13. Hap K, Madziarska K, Hap W, Mazanowska O. Phenotypic risk factors for new-onset diabetes mellitus (NODAT) in renal transplant recipientes. Postepy Hig Med Dosw (online) 2014;68:1347-1351; [ Links ]
14. WHO. Waist circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation, Geneva, 8-11 December 2008. Available at http://apps.who.int/iris/bitstream/10665/44583/1/9789241501491_eng.pdf. Accessed December 20, 2017; [ Links ]
15. Huml AM, Sehgal AR. BMI, sex, and access to transplantation. Clin J Am Soc Nephrol 2014;9:843-844. [ Links ]
Joana da Conceição Silva da Costa
Centro Hospitalar e Universitário de Coimbra
]]> Hospitais da Universidade de Coimbra, Serviço de NefrologiaPraceta Prof. Mota Pinto, 3000-075 Coimbra, Portugal
E-mail: joana.c.s.costa@gmail.com
Disclosure of potential conflicts of interest: none declared.
Received for publication: 12 Jan 2018
Accepted in revised form: 3 Feb, 2018
]]>{kind=link}
{kind=link}
{kind=link}
{kind=link}