Fatores de risco para cicatriz renal após a primeira infeção febril do trato urinário
Risk Factors For Renal Scarring After First Febrile Urinary Tract Infection
Ana Cristina FreitasI; Joana LeiteII; Paula MatosIII; Liliana RochaIII; Teresa CostaIII; Sameiro FariaIII; Conceição MotaIV
I S. de Pediatria Médica do Centro Materno Infantil do Norte, Centro Hospitalar do Porto. 4099-001 Porto, Portugal. anacrisfrei@gmail.com; liliana.oli.rocha@gmail.com;
II S. de Pediatria do Hospital Pedro Hispano. 4464-513 Matosinhos, Portugal. joanamatosleite@gmail.com; ]]>
ABSTRACT
Introduction: The urinary tract infection (UTI) is one of the most common paediatric infectious diseases and it increases the risk for hypertension and end-stage renal disease. Authors aim was to identify risk factors for permanent renal injury after a first febrile urinary tract infection.
Methods: Retrospective analysis of clinical, laboratorial and imaging data of children aged 1 to 36 months hospitalized between January 2010 and December 2012 with the first febrile UTI, comparing with late renal scintigraphy results.
Results: Seventy seven children were included - 53% female, median age of 5 months, Escherichia coli identified in 95%. Renal scintigraphy, performed after the acute episode, revealed renal scars in 19.5%. Cystourethrography was done in 21 patients and vesicoureteral reflux identified in 3. There was no statistically difference between children with and without renal scarring regarding gender, age, body temperature, C-reactive protein, plasmatic creatinine level, bacteriuria or urine nitrite test, urine bacteria identified, presence of vesicoureteral reflux or recurrence rate of UTI.
Conclusions: The authors did not detect any clinical, laboratory or imaging data that may predict progression to renal scarring following a first episode of febrile UTI in children between 1 and 36 months.
]]> Keywords: urinary tract infection, renal scar, renal scintigraphy.RESUMO
Introdução: A infeção do trato urinário (ITU) é uma das doenças infeciosas com maior incidência em Pediatria e apresenta risco de doença renal crónica e hipertensão arterial. O objetivo dos autores foi identificar os fatores de risco para lesão renal após o primeiro episódio de infeção do trato urinário febril.
Métodos: Análise retrospetiva dos dados clínicos, laboratoriais e imagiológicos de crianças entre os 1 e 36 meses de idade, internados entre janeiro de 2010 e dezembro de 2012 por primeiro episódio de ITU febril, comparando os resultados finais da cintigrafia renal.
Resultados: Foram incluídos 77 doentes, dos quais 53% eram do sexo feminino, com idade mediana de 5 meses e com identificação de Eschericia coli em 95%. A cintigrafia renal revelou cicatrizes renais em 19,5% da amostra. A cistouretrografia miccional seriada realizou-se em 21 crianças, tendo-se identificado refluxo vesicoureteral em 3 doentes. Comparando os casos com e sem cicatrizes renais, não se observaram diferenças estatisticamente significativas relativas a género, idade, temperatura corporal, doseamento sérico de proteína C reativa ou creatinina, bacteriúria ou nitritúria, tipo de bactéria identificada, presença de refluxo vesicoureteral ou taxa de recorrência das infeções do trato urinário.
Conclusões: Os autores não detetaram nenhum fator de risco clínico, laboratorial ou imagiológico para progressão para lesão renal após um primeiro episódio de ITU febril em crianças entre 1 e 36 meses.
Palavras-chave: infeção do trato urinário, cicatriz renal, cintigrafia renal.
INTRODUCTION
]]> Urinary tract infection (UTI) is one of the most common infectious diseases in children. The renal parenchyma inflammation and immune reaction in acute pyelonephritis can cause permanent kidney damage with renal scarring.1 The renal scarring extension can subsequently lead to hypertension and end-stage renal disease. In an attempt to optimize follow-up after a febrile UTI, many authors have tried to identify risk factors for renal scarring in these children. The aim of our study was to establish the correlation between the clinical, laboratory and imaging features of the first febrile UTI and the renal scarring formation.
METHODS
This is a retrospective study of children 1 to 36 months of age hospitalized with their first febrile UTI at our paediatric department, between January 2010 and December 2012. Children with known nephrourological or immunological disease were excluded. Febrile UTI was defined as positive urine culture in children with fever and pyuria or positive urine nitrite test. Positive urine culture was defined as: colony-forming units (CFU) ≥ 1 in suprapubic aspiration, CFU ≥ 104 in urine from vesical catheterism or CFU ≥ 105 in urine colleted from middle-stream clean-catch method. At our department, all children from 1 to 36 months age with febrile UTI are submitted to renovesical ultrasound and, after 6 months, to a renal dimercaptosuccinic acid scintigraphy. Those with atypical UTI characteristics (non- response to antibiotics in 48 hours or non-Escherichia coli bacteria identified at urinary culture), recurrent UTI (more than two febrile UTI, three non-febrile UTI or more than one febrile and one non-febrile UTI) or abnormal renovesical ultrasound / renal scintigraphy are submitted to voiding cystourethrography. We analysed the epidemiological characteristics (gender, age, family history of kidney disease), the clinical and laboratory characteristics of febrile UTI (maximum temperature, reactive C protein assay and creatinine, presence of pyuria, nitrituria, bacteriuria and bacteria identified in urine culture), data from the imaging investigation (ultrasound, renal scintigraphy, voiding cystourethrography) and febrile UTI recurrence. These data were then related to the presence of renal scarring in scintigraphy, performed 6 months after the first febrile UTI. Data were analysed using the Statistical Package for Social Science® (SPSS) for Mac version 21 and Microsoft Excell®. There was done a descriptive analysis of patient characteristics and disease evolution and Chi-squared (χ2) test was used as appropriate. The p values of less than 0.05 were considered statistically significant.
RESULTS
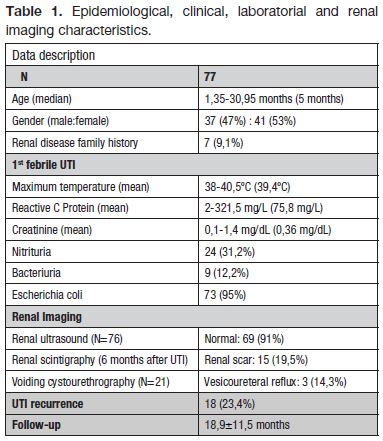
Seventy-seven children were admitted with their first febrile UTI in a period of three years, mostly female (53%) and with a median age of 5 months (1.35-30.95 months). In 9.1% there was a family history of kidney disease, including recurrent UTI, kidney stones, arterial hypertension, polycystic kidney disease and asymmetric renal dimensions.
Clinical, laboratory and renal imaging characteristics are described in Table 1. Escherichia coli was identified in 73 cases, Klebsiella pneumoniae in 2 patients and Proteus mirabilis and Enterococcus faecalis in one case each. Renovesical ultrasound was performed in 76 patients (79% in acute phase), with alterations in 7 patients (9%): duplex kidney, renal asymmetry, nephrocalcinosis, renal malrotation, pyelocaliceal dilation (anteroposterior diameter 5 to 7 mm). Renal scintigraphy detected scarring lesions in 15 patients (19,5%). Voiding cystourethrography was performed in 21 patients, after detecting ultrasound or renal scintigraphy anomalies (12 patients with renal scarring) or identifying non-Eschericia coli in urine culture. Unilateral vesicoureteral reflux (VUR) was detected in 3 patients (grade I, grade III-IV and IV). The case with grade IV vesicoureteral reflux had focal renal lesion on scitigraphy. After 18.9 ± 11.5 months follow up, 23.4% of patients had UTI recurrence.
]]>
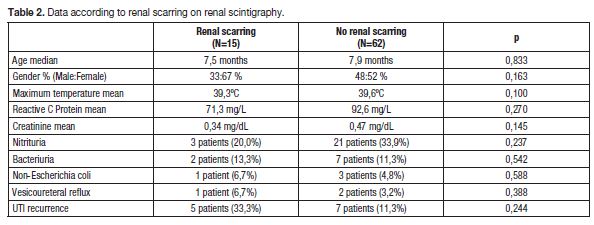
Comparing children with and without renal scarring, we did not found statistically significant difference in any clinical, laboratory or renal imaging data (Table 2). Children with renal scarring had higher recurrent UTI incidence, but the difference had no statistical significance (33% vs. 12%, p = 0.244).
DISCUSSION
Despite the high prevalence of UTI in children there still many doubts about what is the best protocol to use after the first episode. The ideal protocol would identify children who will develop renal scarring by their risk factors, lessening the exposure of non-risk children to the side effects related to its detection. There is a risk of progression to end-stage renal disease associated with the presence of renal scarring, but permanent kidney damage is identified in less than half of children with febrile UTI.2-4 In our department, renal sctintigraphy is performed 6 months after febrile UTI in children between 1 and 36 months. This timing is related to the higher specificity in the detection of renal scarring after 5 months of acute injury to the renal parenchyma.5 In our study, this approach identified renal scarring in 19.5% of children.
Clinical research to identify the risk factors for renal scarring is extensive, in an attempt to optimize the follow-up of these patients. Some authors have identified characteristics that may increase the risk of permanent renal damage, including age, serum inflammation parameters, etiological bacteria, vesicoureteral reflux and UTI recurrence.2, 3, 6-11
One of the most frequently identified risk factor associated with renal scarring is the vesicoureteral reflux. In Shaik et al meta-analysis, VUR had a 2.6 higher risk of renal scarring, which was proportional to the degree of VUR.2 This observation is justified by the presence of retrograde flow of urine carrying potentially infectious agents to the renal parenchyma. However, other authors do not reproduce these results and point that the association of VUR and renal scarring may be influenced by the presence previous renal dysplasia associated with highgrade VUR.4 For this reason we excluded children with known nephrourological disease, in attempt to limit this bias. Our study did not identify any risk factor for renal scarring in children 1 to 36 months with the first febrile UTI. Recently Coutlhard et al have also described the absence of UTI clinical signs that can predict the development of renal scarring.12
The inconsistency and non-reproducibility of the studies keeps the doubts about risk factors and mechanisms leading to persistent renal lesion after the first febrile UTI. This difficulty is due to the different protocols of diagnostic, treatment and follow-up. Our study has the limitations of its sample size and retrospective nature and the lack of a renal scintigraphy in the acute phase in typical UTI. Our results, although contradictory with some studies, are in agreement with our empirical clinical knowledge, which can not identify the children who will progress to renal scaring. In this way, we still maintain renal scintigraphy in the work-up investigation of all febrile UTI in children between 1 and 36 months. It is also important to point out that several molecular and genetic factors and its application in clinical practice remain unclear, so that more research in this area is needed.
]]> CONCLUSION
We found no clinical, laboratory or imaging finding predictive of progression to renal scarring after the first febrile UTI in children between 1 and 36 months.
REFERENCES
1. Vachvanichsanong P. Urinary tract infection: one lingering effect of childhood kidney diseases review of the literature. J Nephrol 2007; 20: 21-8. [ Links ]
2. Shaik N, Ewing A, Bhatnagar S, Hoberman A. Risk of renal scarring in children with a first urinary tract infection: a systematic review. Pediatrics 2010; 126: 1084-90. [ Links ]
3. Oh M, Cheon J, Kang S, Park H, Lee J, Moon D. Predictive factors for acute renal cortical scintigraphic lesion and ultimate scar formation in children with first febrile urinary tract infection. J Urol 2010; 183: 1146-50. [ Links ]
]]>4. Pecile P, Miorin E, Romanello C, Vidal E, Contardo M, Valent F, Tenore A. Age-related renal parenchymal lesions in children with first febrile urinary tract infections. Pediatrics 2009; 124: 23-9. [ Links ]
5. Jakobsson B, Svensson L. Transient pyelonephritic changes on 99mtechnetium-dimercaptosuccinic acid scan for at least five months after infection. Acta Paediatr 1996; 86: 803-907. [ Links ]
6. Preda U, Jodal U, Sixt R, Stokland E, Hansson S. Imaging strategy for infants with urinary tract infection: a new algoritmo. J Urol 2011; 185: 1046-52. [ Links ]
7. Shaik N, Craig J, Rovers M, Da Dalt L, Gardikis S, Hoberman A, et al. Identification of children and adolescentes at risk for renal scarring after a first urinary tract infection: a meta- analysis with individual patient data. JAMA Pediatr 2014; 168: 893-900. [ Links ]
8. Ehsanipour F, Gharouni M, Rafati A, Ardalan M, Bodaghi N, Otoukesh H. Risk factos of renal scars in children with acute pyelonephritis. Braz J Infect Dis 2012; 16: 15-8. [ Links ]
]]>9. Lee Y, Lee J, Park Y. Risk factors for renal scar formation in infants with first episode of acute pyelonephritis: a prospective clinical study. J Urol 2012; 187: 1032-6. [ Links ]
10. Keren R, Shaik N, Pohl H, Graevns-Mueller L, Ivanova A, Zaoutis L, et al. Risk factors for recurrent urinary tract infection and renal scarring. Pediatrics 2015; 136: 13-21. [ Links ]
11. Wennerstrom M, Hansson S, Jodal U, Stokland E. Primary and acquired renal scarring in boys and girls with urinary tract infection. J Pediatr 2000; 136: 30-4. [ Links ]
12. Coulthard M, Lambert H, Keir M. Do systemic symptoms predict the risk of kidney scarring after urinary tract infection? Arch Dis Child 2009; 94: 278-81. [ Links ]
]]> Endereço para correspondência
Email: anacrisfrei@gmail.com
Recebido a 12.11.2015 | Aceite a 01.12.2015
]]>{kind=link}