Imaging case
Caso imagiológico
Fábio BarrosoI; João NascimentoII
I Department of Pediatrics, Centro Materno-Infantil do Norte, Centro Hospitalar do Porto. 4050-371 Massarelos, Portugal. fabiodmb87@gmail.com
II Department of Pediatrics, Hospital Pediátrico de Coimbra, Centro Hospitalar e Universitário de Coimbra. 3000-076 Coimbra, Portugal. nascimentojoao10744@gmail.com
ABSTRACT
Introduction: Calcaneal osteomyelitis is a relatively rare entity and may be underdiagnosed for not being correctly recognized.
Case report: An eight-year-old white boy presented with heel pain and an inability to weight-bearing. The condition was misdiagnosed as Severs disease so he was discharged with symptomatic treatment. Magnetic resonance imaging two weeks after clinical onset revealed diffuse osteomyelitis of his calcaneum. He underwent six weeks of antibiotics administered intravenously, with clinical improvement. In one year of follow-up he has no evidence of complications.
Discussion: Paediatricians should include calcaneal osteomyelitis as a differential diagnosis in any child/adolescent presenting with indolent heel pain. Delays in the diagnosis can lead to disastrous complications.
Keywords: Calcaneal; osteomyelitis; Severs disease
Introdução: A osteomielite do calcâneo é uma entidade clinica relativamente rara e pode ser subdiagnosticada por não ser corretamente reconhecida.
Caso Clínico: Criança de oito anos de idade, raça caucasina, observada no serviço de urgência por dor no calcanhar direito e incapacidade na marcha. Foi inicialmente diagnosticada de doença de Sever, pelo que foi medicada sintomaticamente. A Ressonância Magnética duas semanas após o início da sintomatologia revelou osteomielite difusa de calcâneo. Cumpriu seis semanas de antibioterapia endovenosa com melhoria clínica. No follow-up no ano seguinte, não apresentou evidência de complicações.
]]> Discussão: Os pediatras devem incluir a osteomielite do calcâneo no diagnóstico diferencial da criança/adolescente que apresenta dor indolente do calcanhar. Os atrasos diagnósticos podem conduzir a complicações desastrosas.Palavras-chave: Calcâneo; osteomielite; doença de Sever
An eight-year-old white boy presented with right heel pain and inability to bear weight. There was no preceding history of trauma or wound. He was initially diagnosed as Severs disease due to normal radiographs of the foot. On day two, he developed fever, redness and edema of the right heel, and was discharged with analgesic drugs and limb rest.
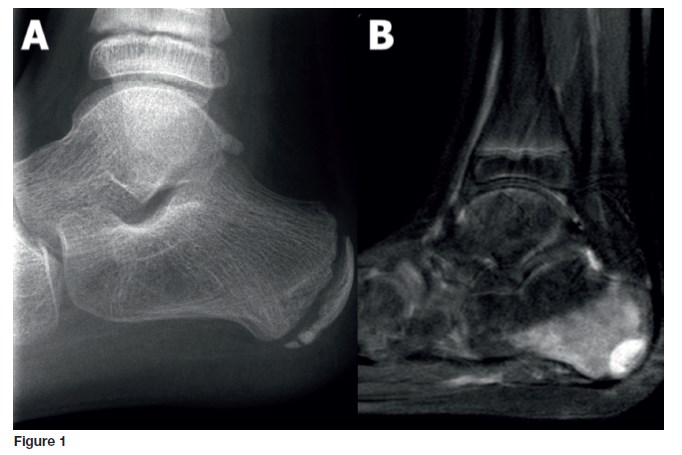
He was admitted to the emergency department after two weeks of increasing heel pain. On physical examination, he presented a 3x3cm posterior calcaneal swelling, redness, tenderness and increased temperature of the right heel. He had a normal white cell count (WCC) and an erythrocyte sedimentation rate of 72mm/hour. Blood cultures were negative. Radiograph on admission showed soft tissue swelling, early rarefaction of the apophysis with no evidence of fracture and magnetic resonance confirmed the presence of osteomyelitis (Figure 1-A and B). He received a six-week course of intravenous flucloxacilin and clindamycin, with gradual clinical improvement. In one year of follow-up he has no evidence of complications.
What is your diagnosis?
DIAGNOSIS
Calcaneal osteomyelitis
]]>DISCUSSION
Calcaneal osteomyelitis is an unusual cause of heel pain in children, often misdiagnosed, representing between 3-10% of all cases of pediatric osteomyelitis.1 It has an insidious presentation comparing to long bone osteomyelitis, affecting usually the posterior aspect adjacent to the apophysis.1,2 It can result from hematologic spread or direct inoculation from a puncture wound (eg. Guthries test) or a foreign body penetration.1-3
The most common responsible agents are Staphylococcus aureus and Pseudomonas aeruginosa.2,3
A unilateral, persistent heel pain with abrupt onset associated with inflammatory signs of the affected heel and inability to bear weight are clues for the diagnosis.3
Plain radiographs can be unreliable in early stages. WCC and serum inflammatory biomarkers are typically borderline but ESR showed to be more reliable.3,4
Antibiotic treatment is similar to long bone osteomyelitis and it should be performed from four to six weeks. Attending to the lack of evidence, early surgical debridement and biopsy are not recommended for routine.5 Diagnosis delay can result in chronic osteomyelitis, ankylosis, growth arrest and deformity.2,4
REFERENCES
1. Chen K, Balloch R. Management of calcaneal osteomyelitis. Clin Podiatr Med Surg. 2010; 27:417-29. [ Links ]
2. Mallia et al. Delayed recognition of pediatric calcaneal osteomyelitis: a case report. Journal of Medical Case Reports. 2015; 9:185. [ Links ]
3. Puffinbarger W. et al. Osteomyelitis of the calcaneus in children. J Pediatr Orthop. 1996; 16: 22430. [ Links ]
4. Jaakkola J, Kehl D. Hematogenous calcaneal osteomyelitis in children. J Pediatr Orthop. 1999; 19:699708. [ Links ]
5. Hamdy R. et al. Subacute hematogenous osteomyelitis: are biopsy and surgery always indicated? J Pediatr Orthop. 1996; 16:2203. [ Links ]
]]> CORRESPONDENCE TO
Received for publication: 03.02.2017 Accepted in revised form: 06.03.2017
]]>{kind=link}