Caso estomatológico
Oral pathology case
José M. S. AmorimI
I Department of Stomatology and Maxillofacial Surgery, Pediatric Unit, Centro Hospitalar do Porto. 4099-001 Porto, Portugal. joseamorim.dia@chporto.min-saude.pt
]]>
RESUMO
Adolescente de 12 anos referenciado à consulta de Estomatologia Pediátrica devido a não erupção do dente incisivo central superior esquerdo. Ao exame objetivo apresentava agenesia de 21, bem como abaulamento da cortical vestibular na região da inclusão. Realizou OPG e TAC maxilar, que evidenciou inclusão do dente 21 com quisto (provavelmente dentígero) envolvendo o mesmo e ainda a presença de um mesiodens incluso.
Realizou enucleação da lesão quística, bem como extração do incisivo associado e do mesiodens, tendo-se preenchido a cavidade com substituto de osso e isolado com membrana.
Palavras-chave: Enucleação cística; imagem radiolúcida; inclusão de mesiodens; quisto dentígeno odontogénico
ABSTRACT
An 12-year-old boy was referred to the Pediatric Stomatology Clinic for absence of eruption of permanent maxillary left incisive tooth. Physical examination revealed bulging of the vestibular cortical bone of the 2nd quadrant, agenesis of the tooth 21.
Physical examination: Orthopantomography and CT scan of the upper jaw revealed a large radiolucent image that occupied the maxillary sinus and tooth 2.1 within the cyst and the presence of a mesiodens included.
A presumptive diagnosis of an odontogenic dentigerous cyst was made.
]]> Treatment procedure comprised cystic enucleation with extraction of 2.1. The bone defect was filled with bone substitute (Geistlich Bio-Oss) and collagen membrane (Geistlich Bio-Gide).Keywords: Cystic enucleation; mesiodens included; odontogenic dentigerous cyst; radiolucent image
A 12-year-old male was referred to the Pediatric Stomatology clinic, due to the non-appearance of the tooth 21 in the left maxillary arch and swelling of the vestibular cortical bone in the region of the non-erupted tooth.
Personal and family history were irrelevant.
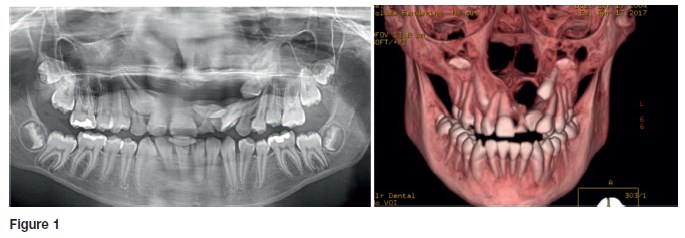
Physical examination revealed painless, soft and depressible bulging of the vestibular cortical bone of the 2nd quadrant, without fistula; agenesis of the tooth 21, with contralateral incisor tooth (11) completely erupted, no dental caries; no gingivitis. Orthopantomography (OPG) showed a large radiolucent image, occupying an important part of the maxillary sinus, with the tooth 21 included and a supernumerary tooth included in space 11-21. To assess correct evaluation of the limits and dimension of the cyst Maxillary computerized tomography (MCT) was performed (Fig.1).
What is your Diagnosis?
What is your clinical management?
]]> DISCUSSION
The clinical case report is an odontogenic cyst probably dentigerous, as well as the presence of a supernumerary tooth - mesiodens.
Odontogenic cysts are divided into two major groups: developmental and inflammatory cysts. In the group of developmental cysts, the dentigerous cysts are the most frequent, and they are always associated with an included tooth; this clinical situation is very frequent in the maxilla.
The dentigerous odontogenic cyst is defined radiologically as a radiolucent image associated with an included tooth and may have very variable dimensions when they have free space to expand (for example, for the maxillary sinus).
Whenever a tooth does not make its appearance in the dental arcade in the expected time and a dental cyst or dental inclusion is suspected, the request of a OPG is the correct procedure.
These cysts are rare in the deciduous dentition and are commonly associated with the most frequently included teeth: third molars and maxillary canines. The inclusion of incisor teeth is not a frequent clinical situation. They occur mostly in males with no ethnicity predominance
Treatment is always surgical and consists on cystic enucleation, as well as the extraction of the included tooth. In some clinical situations the cyst is marsupialized to reduce its size before it is enucleated. In the present case the bone defect was filled with bone substitute (Geistlich Bio-Oss) and collagen membrane (Geistlich Bio-Gide).
The histological study confirmed the clinical suspicion of dentigerous cyst.
The prognosis is good. The mesiodens is the most common supernumerary tooth in the dental maxillary arch, located in the midline of the maxilla, between the upper central incisors.
When a definitive maxillary central incisor tooth does not make its appearance in the dental arch at the expected time, either the tooth does not exist (dental agenesis), or there is a supernumerary tooth that prevents the eruption of the definitive tooth.
]]> Orthopantomography is the most habitual radiographic investigation to visualize supernumerary teeth.The treatment plan consists of extraction of the supernumerary tooth and regular observation to monitor proper eruption and alignment of the definitive tooth.
REFERÊNCIAS BIBLIOGRÁFICAS
1. Cawson RA, Odell EW. Cawson´s Essencials of Oral Pathology and Oral Medicine. 17th London: Elsevier Health Sciences; 2002. p.108-10 [ Links ]
2. Leache EB. Odontopediatría. Barcelona: Masson; 2003. p. 60-8. [ Links ]
3. Regezi JA, Sciubla JJ, Pogrel MA. Atlas of Oral and Maxillofacial Pathology. 1nd. Philadelphia: Saunders; 2000. p. 147. [ Links ]
]]> CORRESPONDENCE TO
José M. S. Amorim
Department of Stomatology and Maxillofacial Surgery
Pediatric Unit
Centro Hospitalar do Porto.
Largo do Prof. Abel Salazar,
4099-001 Porto
Email: joseamorim.dia@chporto.min-saude.pt
Received for publication: 04.09.2017 Accepted in revised form: 11.09.2017
]]>{kind=link}