ARTIGOS ORIGINAIS | ORIGINAL ARTICLES
Subclinical Hypothyroidism in Children and Adolescents: a single-center retrospective study
Hipotiroidismo Subclínico em Crianças e Adolescentes: estudo retrospetivo de um centro terciário
Ana Margarida MonteiroI; Maria Miguel GomesII; Olinda MarquesI,III; Ana AntunesIII; Sofia A. MartinsIII
I Department of Endocrinology, Hospital de Braga. 4710-243 Braga, Portugal. anamargaridacmonteiro@gmail.com; opmarques@netcabo.pt ]]>
II Department of Pediatrics, Hospital de Braga. 4710-243 Braga, Portugal. mariamgomes@hotmail.com
ABSTRACT
Introduction: The ideal management of subclinical hypothyroidism, particularly the mild form, remains unclear. Our objectives were to describe the clinical management of subclinical hypothyroidism in children and adolescents and the natural course of the disease with conservative management.
Material and Methods: We retrospectively analyzed clinical records of patients, under the age of 18 years, referred to our pediatric endocrinology department due to subclinical hypothyroidism between 2009 and 2014, with ≥1 year of follow-up. Patients under one month of age and with TSH (thyroid-stimulating hormone) levels <5 uUI/mL were excluded. Subclinical hypothyroidism was considered when TSH levels >5 uUI/mL with a normal serum free thyroxine. Mild and severe subclinical hypothyroidism were defined when TSH was <10 uUI/mL and ≥10 uUI/mL, respectively.
Results: We included 69 patients (62.3% girls) with a median age at diagnosis of 8.0 [(25th percentile-75th percentile (P25-P75): 4.75-11.0)] years. Most of the patients (80.6%) were symptomatic and Hashimoto thyroiditis was the most frequent identified cause. A mild form of subclinical hypothyroidism was diagnosed in 79.7% of the patients. All patients with severe subclinical hypothyroidism initiated therapy with levothyroxine in contrast with 43.6% in the mild subclinical hypothyroidism group. Among patients not treated, 73.3% had TSH normalized after one year of follow-up and none progressed to overt hypothyroidism.
Conclusion: The mild form of subclinical hypothyroidism was the most common type pf disease and, among patients managed conservatively, the majority presented normal thyroid function after one year of follow-up and none progressed to overt hypothyroidism. Our results reinforce the idea that, in most patients, subclinical hypothyroidism is a benign condition with a low risk of progression to overt thyroid dysfunction. However, further studies are needed to evaluate the potential long-term effects of the condition in untreated patients and to clarify the best clinical approach and follow-up strategy.
Keywords: Childhood; levothyroxine treatment; subclinical hypothyroidism
Introdução: A orientação do hipotiroidismo subclínico, particularmente a forma leve, permanece indefinida. Os nossos objetivos foram avaliar a orientação do hipotiroidismo subclínico em crianças e adolescentes e o curso natural em doentes seguidos de forma conservadora.
Material e Métodos: Foram analisados retrospetivamente os registos clínicos de doentes com idade inferior a 18 anos, encaminhados ao nosso departamento de endocrinologia pediátrica por hipotiroidismo subclínico entre 2009 e 2014, com ≥1 ano de acompanhamento médico. Foram excluídos doentes com idade <1 mês e níveis de TSH (thyroid-stimulating hormone) <5 uUI/mL. O hipotiroidismo subclínico foi considerado quando níveis de TSH> 5 uUI/mL com tiroxina livre sérica normal. Hipotiroidismo subclínico leve e grave foram definidos para valores de TSH <10 uUI/mL e ≥ 10 uUI/mL, respetivamente.
Resultados: Foram avaliados 69 doentes (62,3% eram meninas) com uma idade mediana ao diagnóstico de 8,0 anos [(percentil 25 - percentil 75 (P25-P75): 4.75-11.0) anos )]. A maioria dos doentes (80,6%) apresentava sintomas e a tiroidite de Hashimoto foi a causa mais frequentemente identificada. A forma leve de hipotiroidismo subclínico foi diagnosticada em 79,7% dos doentes. Todos os doentes com hipotiroidismo subclínico grave iniciaram levotiroxina, em contraste com 43,6% em doentes com hipotiroidismo subclínico leve. Entre os doentes não tratados, 73,3% tinham TSH normalizada após um ano de acompanhamento e nenhum evoluiu para hipotiroidismo evidente.
Conclusão: A forma leve de hipotiroidismo subclínico foi a mais comum e, entre os doentes seguidos de forma conservadora, a maioria apresentou normalização da função tiroideu um ano após o acompanhamento e nenhum evoluiu para hipotiroidismo. Os nossos resultados reforçam o conceito de que, na maioria dos doentes, o hipotiroidismo subclínico é uma condição benigna com baixo risco de progressão para hipotiroidismo. No entanto, são necessários estudos adicionais para avaliar os potenciais efeitos a longo prazo em doentes não tratados e esclarecer o melhor acompanhamento clínico.
Palavras-chave: Hipotiroidismo subclínico; infância; tratamento com levotiroxina
INTRODUCTION
Subclinical hypothyroidism (SCH) is defined by serum thyroid-stimulating hormone (TSH) levels above the upper limit of the reference range in the presence of normal serum concentrations of thyroxine (T4) (both total and free T4). Despite the dynamic changes in the thyroid function known to occurs in the newborn period, a serum TSH concentration above 5 uUI/mL can be considered abnormal after one month of age, when modern third-generation assays are used.1
]]> The available data from epidemiological studies conducted in children and adolescents are limited and the estimated prevalence of SCH in children is less than 2%. Multiple etiologic factors are implicated in the development of SCH during childhood but Hashimoto thyroiditis (HT) is usually reported as the most frequent cause.1Increases in serum TSH levels might be indicative of mild hypothyroidism and, consequently, of a reduced action of thyroid hormones on the peripheral tissues. During infancy and childhood, functional abnormalities of the thyroid gland can adversely affect growth and brain maturation with clinical consequences depending on age and the severity of thyroid impairment. Nevertheless, the association between SCH in childhood and adverse health outcomes remains controversial.2 It has been demonstrated that SCH is a benign condition and that most of the patients with SCH revert to euthyroidism or remain with SCH with a low risk of progression to overt thyroid dysfunction.3 Conversely, emerging evidence has demonstrated that modest increases in the levels of TSH might be associated with subtle cardiometabolic abnormalities in childhood and adolescence.46
The management of SCH remains unclear, particularly regarding the mild form of disease. The decision about whether to treat or not these patients, should be made after careful discussion with the parents of the risks and potential benefits of the treatment. At present, there is insufficient evidence to recommend treatment in the majority of children with SCH with serum TSH concentrations under 10 uUI/mL.1
We aimed to describe the etiology and the clinical management of SCH in children and adolescents followed in our center between 2009 and 2014. We also intended to compare clinical characteristics between patients with mild and severe forms of SCH, as well as the natural course of SCH in patients treated and not treated with levothyroxine.
MATERIAL AND METHODS
Patients and data collection
We retrospectively analyzed the clinical records of children and adolescents referred to our pediatric endocrinology outpatient center with suspected SCH, between 2009 and 2014. We include in the present analysis all patients with at least one year of follow-up. Patients under one month of age (n=2) and patients with TSH levels below 5 uUI/mL (n=33) were excluded.
Several personal and clinical variables were recorded, such as gender, age at presentation of SCH, anthropometric data (height and weight) and pubertal stage (pre-pubertal or pubertal). Serum concentrations of thyroid-stimulating hormone (TSH), free thyroxine (fT4), titer of anti-thyroid autoantibodies: antiperoxidase (anti-TPO) and antithyroglobulin (anti-Tg), were performed at diagnosis and at least once a year. We also evaluated the presence of clinical symptoms suggesting thyroid disease (weight gain, fatigue, constipation or modifications in growth velocity, body weight or psychomotor development), thyroid ultrasound findings, associated comorbidities and family history of thyroid disease.
Definitions
]]> SCH was considered if TSH levels were above 5 uUI/mL with a normal serum fT4 concentration.1 Mild and severe SCH were defined when TSH was inferior or equal/superior to 10 uUI/mL, respectively.Hashimoto thyroiditis (HT) was diagnosed if positive thyroid auto-antibodies (anti-TPO and/or anti-Tg) and/or ultrasound findings suggestive of thyroiditis (diffuse heterogenicity and/or pseudonodularities and/or hypoechoic micronodules) were present.
Body mass index (BMI)-for-age values were classified according to the World Health Organization (WHO) reference data: overweight was considered if BMI was ≥ 85th percentile and obesity if BMI was ≥ 97th percentile.
Statistical analysis
Statistical analyses were performed with the program IBM SSPS version 20. Normal distribution of the variables was evaluated using the KolmogorovSmirnov test. Differences between groups in continuous variables were performed using Students T tests (normal distribution) and Mann-Whitney tests (non-normal distribution) and in categorical variables using χ2 test. Statistical significance was accepted at the level of p <0.05.
RESULTS
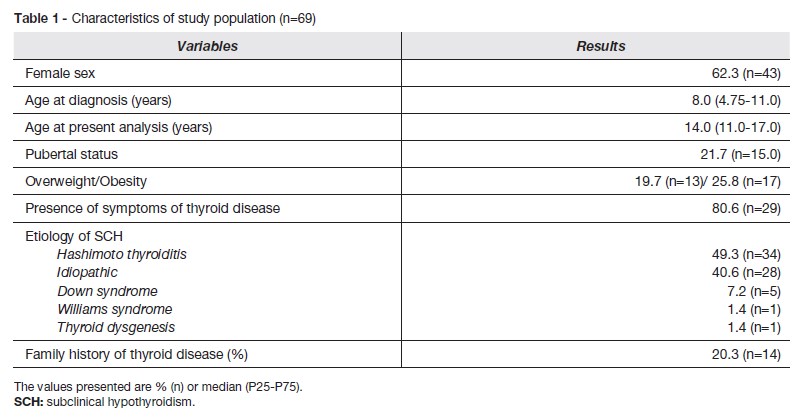
A total of 69 children (62.3% girls) and adolescents were included with a median follow-up of 3.0 (P25-P75: 2.0-3.0) years and a median age at diagnosis of 8.0 (P25-P75: 4.75-11.0) years. Almost half of the children were overweight and 25.8% were considered obese. The general characteristics of the study population are described in table 1.
The most frequent reasons described for thyroid function testing were changes in body weight (24.6%; n=17), diminished growth velocity (7.2%; n=5) and palpable thyroid nodules (5.8%; n=4).
Autoimmune diseases were present in 14.5% (n=10) of the patients (5 type 1 diabetes, 2 coeliac disease, 1 Addison disease, 1 psoriatic spondylitis and 1 scleroderma). Down syndrome was present in 14.5% (n=10) of the patients. In 17.4% (n=12), only obesity was present and in 37.7% (n=26) no comorbidities were described. As shown in table 1, HT was the principal etiology of SCH.
]]> Most of the patients had a mild form of SCH (79.7%; n=55) while 20.3% (n=14) presented a severe form of SCH. All patients with severe SCH initiated therapy with levothyroxine in contrast with 43.6% patients in mild SCH group (100.0% vs 43.6%; p<0.001). Other clinical differences between these two groups are presented in table 2.Among treated patients, 83.3% (n=31) achieved a normal TSH within 3 to 6 months of levothyroxine therapy and the median (P25-P75) dose of levothyroxine was 1.3 (0.9-2.0) mcg/kg/day.
We found that patients with alterations on thyroid ultrasound were more frequently treated with levothyroxine (56.7% vs 17.6%; p=0.009). However, no differences in age, gender and presence of symptoms or presence of HT were found between patients with or without levothyroxine therapy.
From a total of 31 patients not treated with levothyroxine, 73.3% (n=22) had a normal TSH after one year of follow-up. At two and three years of follow-up, 74.1% (n=20) and 90% (n=18) achieved euthyroidism respectively. In this group no patient progressed to overt hypothyroidism during the follow-up period. In patients with resolved SCH after one year, there were no differences between the presence or absence of HT (45.5% vs 54.5%; p=0.200).
DISCUSSION
In our study, most patients with SCH were symptomatic and the mild form of SCH was the most common. Among patients managed conservatively the majority had normal thyroid function after one year of follow-up and none progress to overt hypothyroidism.
According to similar studies, we verified that most patients were girls.7,8 This may reflect the elevated prevalence of HT in our group study, as it is more frequent in female gender.9
The reasons for initial thyroid function request were diverse. The increasing number of children undergoing thyroid testing even in the absence of newly detected goiter, thyroid nodules or classic symptoms of thyroid dysfunction contribute to this diversity. Actually, thyroid tests are often ordered as part of an evaluation for overweight or obesity, in the work-up of fatigue with no goiter and no other symptoms of hypothyroidism, in children with a family history of hypothyroidism, in short healthy children with normal growth rates, as well as in children with precocious or delayed puberty.10
When questioned, most patients presented with at least one symptom of thyroid dysfunction or a sign that leaded to thyroid dysfunction suspicion. There was a similar prevalence of symptomatic patients in the study of Such et al.8 However, Lee et al reported no symptomatic patients.7 These findings are controversial as symptoms of hypothyroidism are neither sensitive nor specific and they dependent on the clinician subjectivity and report.
]]> We found that the most of the children and adolescence had other comorbidities. The most frequent reported were autoimmune disorders, particularly type 1 diabetes and Down syndrome. In fact, some genetic syndromes, such as Down syndrome, are susceptible to subclinical hypothyroidism associated or not with HT. As HT is an autoimmune disease, it tends to cluster in the same patient and in the family. This fact also explains the positive family history of thyroid disease reported in about 20% of the patients. 2,9 Interesting, in the study of Rapa et al, almost half of the patients with idiopathic SCH had a positive family history of thyroid diseases, which was justified by a higher prevalence of nonsynonymous mutations in the TSH-receptor gene.11Almost half of the children were overweight and 25.8% was considered obese. The relationship between obesity and subclinical hypothyroidism in childhood remains not defined. There is evidence suggesting that elevation of TSH concentration is a consequence rather than a cause, as it might represent an adaptation of the hypothalamicpituitarythyroid axis to obesity. Accordingly, TSH levels among children with obesity tend to decrease with weight loss induced by lifestyle changes.2
In concordance with the published literature, in our population, HT was the most frequent cause of SCH followed by idiopathic SCH.13,12
In this retrospective study, we aimed to evaluate the management of SCH in children and adolescents, as it remains a controversial topic. The severe form of SCH was documented in about 20% of the patients and all initiated therapy with levothyroxine.
According to the European Thyroid Association, the decision to treat should be made after careful discussion with the parents informing the risks and potential benefits of treatment. Also, they pointed to an insufficient evidence to recommend treatment in the majority of children with SCH in whom the serum TSH concentration is inferior to 10 uUI/mL. 1 In a recent review, Salerno et al proposed that the final decision on treatment should be made according to the presence of clinical symptoms or signs of mild thyroid impairment and the risk of progression to overt hypothyroidism. Accordingly, treatment with levothyroxine should be considered for all children affected by severe forms (TSH levels > 10 uUI/mL) or in those with mild SCH in the presence of goitre or the signs or symptoms of hypothyroidism. For children with mild forms, a trial of levothyroxine can be considered if there is a clinical suspicion of hypothyroidism. In the absence of signs and symptoms, regular clinical evaluation of TSH and fT4 levels, along with periodic revaluation of anti-thyroid antibodies, is advisable.2
In our center, 43.6% patients with mild SCH were treated with levothyroxine. We found that patients with thyroid ultrasound alterations were more frequently treated with levothyroxine, however, no differences in age, gender, presence of symptoms or presence of HT were found. These findings suggest that, in our clinical center, the pediatric endocrinologists decisions were based on their own experience and, possibly, on suggestive ultrasound findings of thyroid disease. Between patients with conservative management (not treated with levothyroxine), the majority had their TSH normalized after one to three years of follow-up. These results are in concordance with published similar studies, despite the variability of the natural history of SCH depending on its etiology.3 SCH in childhood seems to be a benign and remitting condition. Currently, there is no evidence of alterations in growth or neurocognitive development in patients with mild untreated SCH. However, ongoing studies have highlighted the presence of subtle pro-atherogenic abnormalities among children with modest increases in TSH levels and have suggested an improvement of these parameters after treatment with levothyroxine. Although these findings are not sufficient to support treatment for children with mild asymptomatic forms, they should draw attention to the need of cardiovascular risk assessment among those patients. To address the long-term benefits and risks of levothyroxine treatment among children and adolescents with mild SCH, adequate randomized controlled trials are needed.
The main limitation of our study was its retrospective character, along with the limited number of patients evaluated. Besides, most of the patients were followed-up for a short period of time. On the other hand, we sought to address a controversial topic with limited evidence and reinforce the necessity of further studies, particularly prospective randomized trials. Furthermore, the retrospective analysis allowed for an audit of the procedures and subsequent reflection.
CONCLUSIONS
Our results reinforce the idea that, in most patients, SCH is a benign condition with a low risk of progression to overt thyroid dysfunction. However, further studies are needed to evaluate the potential long-term effects in untreated patients and clarify the best clinical follow-up.
]]>REFERÊNCIAS BIBLIOGRÁFICAS
Lazarus J, Brown RS, Daumerie C, Hubalewska-Dydejczyk A, Negro R, Vaidya B. 2014 European thyroid association guidelines for the management of subclinical hypothyroidism in pregnancy and in children. Eur Thyroid J. 2014; 3:76-94. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=4109520&tool=pmcentrez&rendertype=abstract.
Salerno M, Capalbo D, Cerbone M, De Luca F. Subclinical hypothyroidism in childhood - current knowledge and open issues. Nat Rev Endocrinol. 2016; 12:734-746. doi: 10.1038/nrendo.2016.100.
Monzani A, Prodam F, Rapa A, Moia S, Agarla V, Bellone S, et al. Endocrine disorders in childhood and adolescence. Natural history of subclinical hypothyroidism in children and adolescents and potential effects of replacement therapy: a review. Eur J Endocrinol. 2013; 168:111.
Cerbone M, Capalbo D, Wasniewska M, Raso GM, Alfano S, Meli R, et al. Cardiovascular risk factors in children with long-standing untreated idiopathic subclinical hypothyroidism. J Clin Endocrinol Metab. 2014; 99:2697703.
Sert A, Pirgon O, Aypar E, Yilmaz H, Odabas D. Subclinical Hypothyroidism as a Risk Factor for the Development of Cardiovascular Disease in Obese Adolescents With Nonalcoholic Fatty Liver Disease. Pediatr Cardiol. 2013;1-9.
Unal E, Akın A, Yıldırım R, Demir V, Yıldız İ, Haspolat YK. Subclinical hypothyroidism in children may lead to dyslipidemia and increased carotid intima-media thickness. J Clin Res Pediatr Endocrinol. 2016. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28008862
Lee YJ, Jung SY, Jung HW, Kim SY, Lee YA, Lee SY, et al. Unfavorable Course of Subclinical Hypothyroidism in Children with Hashimotos Thyroiditis Compared to Those with Isolated Non-Autoimmune Hyperthyrotropinemia. J Korean Med Sci. 2017; 32:124. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27914141
Such K, Gawlik A, Dejner A, Wasniewska M, Zachurzok A, Antosz A, et al. Evaluation of Subclinical Hypothyroidism in Children and Adolescents: A Single-Center Study. Int J Endocrinol. Hindawi Publishing Corporation. 2016.
Radetti G. Clinical Aspects of Hashimotos Thyroiditis. In: Endocrine development. 2014: 15870. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25231451
Kaplowitz PB. Subclinical hypothyroidism in children: normal variation or sign of a failing thyroid gland? Int J Pediatr Endocrinol. 2010; 2010:281453. doi: 10.1155/2010/281453.
Rapa A, Monzani A, Moia S, Vivenza D, Bellone S, Petri A, et al. Subclinical hypothyroidism in children and adolescents: a wide range of clinical, biochemical, and genetic factors involved. J Clin Endocrinol Metab. 2009; 94:241420.
Radetti G, Maselli M, Buzi F, Corrias A, Mussa A, Cambiaso P, et al. The natural history of the normal/mild elevated TSH serum levels in children and adolescents with Hashimotos thyroiditis and isolated hyperthyrotropinaemia: A 3-year follow-up. Clin Endocrinol. 2012; 76:3948.
CORRESPONDENCE TO
Ana Margarida Monteiro ]]>
Department of EndocrinologyReceived for publication: 28.04.2017 Accepted in revised form: 11.07.2017
]]>{kind=link}