
QUAL O SEU DIAGNÓSTICO? | WHAT IS YOUR DIAGNOSIS?
Imaging case
Caso imagiológico
Maria Adriana RangelI, Graça LoureiroII, Mariana PintoII
I Department of Pediatrics, Centro Hospitalar de Vila Nova de Gaia e Espinho. 4400-129 Vila Nova de Gaia, Portugal. mariaadrianarangel@hotmail.com ]]>
II Department of Pediatrics, Centro Hospitalar Entre Douro e Vouga. 4520-161 Santa Maria da Feira, Portugal. mariagracaloureiro@gmail.com; marianabrpinto@gmail.com Correspondence to
ABSTRACT
Introduction: Cephalohematoma is a collection of serosanguineous fluid below the periosteum and is the most frequent cranial injury in the newborn, occurring in 0.2-2.5% live births. The majority of cephalohematomas spontaneously resolve within three to four weeks, however, some persist beyond four weeks and begin to calcify.
Case report: A seven-week-old boy, was referred to the emergency department because of a head lump on the right parietal region, with no other symptoms. He was born after a vacuum-assisted delivery, and presented a cephalohematoma in the first days of life, that progressively decreased and became more rigid. Physical examination, revealed a cranial asymmetry, and a head lump on the right parietal region, that was hard and fixed to the bone. Head X-ray revealed a radiopaque lump on the right parietal bone and a poorly defined arched line, as well as visible microcalcifications on the core of the cephalohematoma, typical findings of a calcified cephalohematoma.
Discussion: Even though cephalohematoma is frequently encountered, calcified cephalohematoma is seen only sporadically, and is a rare clinical entity. History and clinical examination are important in the differential diagnosis and imaging strategy. Radiography and ultrasonography are often the initial screening diagnostic tests, followed by magnetic resonance imaging or computed tomography. Head x-ray features, in this case report, where particularly evocative of the diagnosis.
Keywords: Birth Injuries; calcified cephalohematoma; newborn
RESUMO
Introdução: O cephalohematoma é uma coleção sero-hemática subperióssea e é o traumatismo craniano mais frequente do recém-nascido, ocorrendo em 0,2-2,5% dos nados vivos. A maioria sofre regressão espontânea pelas três a quatro semanas de vida, sendo que uma minoria persiste após as quatro semanas, podendo evoluir para calcificação.
]]> Caso Clínico: Lactente de sete semanas, sexo masculino, referenciado ao serviço de urgência por tumefação craniana na região parietal direita. Nascido de parto distócico por ventosa; observou-se cefalohematoma nos primeiros dias de vida, o qual diminuiu progressivamente de tamanho, tornando-se mais rígido. Sem qualquer outra sintomatologia. Ao exame físico era notória, uma assimetria craniana e uma tumefação na região parietal direita, dura e fixa à palpação do crânio. A radiografia de crânio revelou uma tumefação radiopaca parietal direita, associada a uma linha arqueada mal definida, bem como microcalcificações na parte central do cefalohematoma, achados típicos de um cefalohematoma calcificado.Conclusão: Embora o cefalohematoma seja frequentemente observado, o cefalohematoma calcificado é visto apenas esporadicamente e é uma entidade clínica rara. A história clinica e exame físico são importantes para o diagnóstico diferencial e planificação do estudo imagiológico. A radiografia e a ecografia são habitualmente os exames de primeira linha seguidas pela ressonância magnética ou tomografia computorizada. As características da radiografia de crânio, neste caso clínico, foram particularmente sugestivas do diagnóstico.
Palavras-chave: Cefalohematoma calcificado; recém-nascido; traumatismos do nascimento
A seven-week-old boy was referred for presenting a hard mass over the right parietal region of the skull. A soft swelling was present in the first few days of life, that progressively decreased in size and became more rigid. No other symptoms were reported, namely irritability, vomiting or fever. The baby was the first born of non-consanguineous healthy parents. Pregnancy was monitored and uneventful and the baby was born at 38 weeks through vacuum-assisted delivery, with an Apgar score of 9/10 by the 1st/5th minute. He presented a cephalohematoma, localized at the region of attachment of the suction cup. Neonatal period was otherwise uneventful. There was no history of trauma besides the cephalohematoma at birth or other pathological process such as bleeding disorders.
On physical examination he was calm, with appropriate toning and reflex. A cranial asymmetry was notorious, with a visible head lump (figure 1) on the right parietal region, hard and fixed to the bone. There was no associated soft tissue abnormality, and the margins were indistinct. The scalp was freely moving over the swelling and apparently painless, since there was no grimace of pain or crying during palpation. Remaining physical examination unremarkable.
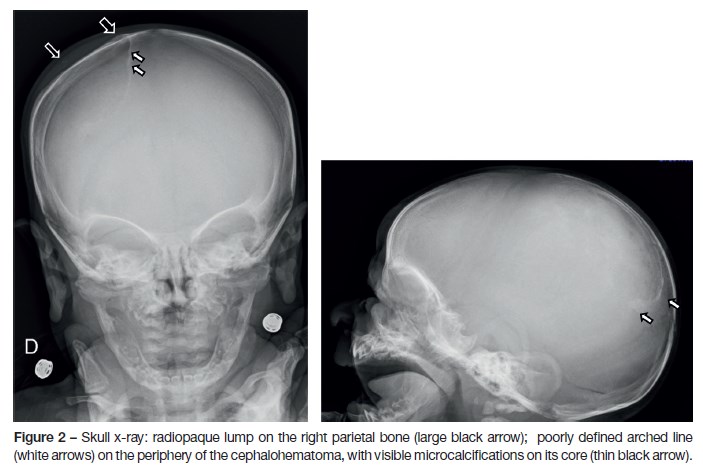
A head X-ray (figure 2) revealed a radiopaque lump on the right parietal bone (large black arrow) and a poorly defined arched line (white arrows) on the periphery of the cephalohematoma, with visible microcalcifications on its core (thin black arrow). No cranial fracture was seen.
What is your diagnosis?
DIAGNOSIS
Calcified cephalohematoma (CC)
DISCUSSION
Birth injuries to the head occur because the head is particularly vulnerable to trauma during vertex delivery.1 Cephalohematoma is the most frequent cranial injury in the newborn, occurring in 0.2-2.5% live births, with parietal bone being the most common site of involvement.2,3 However there are reports of diagnosis in útero by prenatal ultrasound or after cesarean section.1
Cephalohematoma is a collection of serosanguineous or bloody fluid below the periosteum of the skull. It results from bleeding of the emissary and diploic veins into the subperiostial layer. The bleeding is contained by the ligaments that attach the periosteum to the skull at the cranial suture lines. The pressure in this area builds and acts as a tamponade to stop further bleeding. However, as it occurs in a deeper and more vascular portion of the scalp, it usually has a higher content of blood than caput succedaneum.1
]]> Clinically, cephalohematoma is not usually present at birth but develop hours or even days after delivery, as an immobile, firm, localized mass with cranial sutures clearly defining the boundaries.1,4 It occurs more frequently in primigravidas, in male gender or macrosomic newborns, in instrumented assisted deliveries (vacuum or forceps), prolonged difficult labour, cephalopelvic disproportion, head in deviant position (occipital transverse) or when a scalp electrode has been placed.1Complications of cephalohematoma may include: anaemia (albeit rare) and hyperbilirubinemia (due to resolving hematoma); underlined linear skull fractures (5-20%); or rarely meningitis, osteomyelitis or intracranial injury.4
The majority of cephalohematomas spontaneously resorb, by gradual haemolysis; the swelling becomes increasingly fluctuant and generally resolves in three to four weeks.3,4 In about 3-5% of cases, cephalohematoma persist beyond four weeks and progresses to calcification.2,3 This results from a process of subperiostial osteogenesis and calcium deposits in the area. The calcification process begins when a ridge forms along the periphery of the hematoma, causing distortion of the calvaria.2 The rate of sub-pericranium osteogenesis is variable.3 If sufficiently large, the hematoma can depress the malleable neonatal skull, causing it to encroach into the cranial vault space as the cephalohematoma expands. This supports the current classification of Calcified Cephalohematoma (CC) in two types: type 1, non-depressed with no encroachment into the cranial cavity; and type 2, depression of the inner bone and encroachment. This classification is important as it determines the appropriate corrective surgical technique.3
Although rare, calcified or ossified cephalohematomas can cause significant deformities to the skull requiring treatment. Besides the aesthetic effects, clinical sequelae are rarely reported (even in type 2 CC), however, electroencephalography anomalies have been reported, and association with sagittal synostosis, although this is not clear and still subject of debate.2,5 While there are currently no reported cases of CC causing focal neurological deficits or disturbances in intracranial pressures, the long-term effects of a calcified mass encroaching into the cranial vault (in type 2 CC) on brain development is unknown.3
Neuroimaging is the main investigation needed for CC. Duplex/color doppler ultrasound (US) in the evaluation of head bumps and lumps provides rapid acquisition of information including size, shape, location, internal content and vascularity.6,7 This imaging technique does not expose patients to radiation or iodinated contrast nor requires sedation. Skull X-ray features includes an expansible lesion surrounded by a radio-opaque rim, as seen in this case (figure 2).3 There may be a variable thinning of the underlying calvarium.3 CT-Neuroimaging may be needed to exclude a deformation of the inner carinal surface, for assessment of type of lesion and for operative planning. It may also be useful for differential diagnosis such as bone tumour or scalloping of skull due to brain tumours/lesions and to exclude an intracranial hematoma.2 Despite the use of radiation, CT is the standard for assessment of CC.7 Its features include a uniformly homogenous, hypodense, non-enhancing core encased by bone.3 Three-dimensional reconstructive CT allows preoperative planning of appropriate reconstructive technique.2 On Magnetic Resonance Imaging (MRI), cephalohematoma exhibits a bright signal on T1-weighted images and a predominantly high signal with mild heterogeneity on T2-weighted images, due to the presence of methaemoglobin, indicating that the lesion is secondary to haemorrhage rather than to an intraosseous tumor.2,3
After ossification, cephalohematoma may undergo spontaneous remodelling and disappear within three to six months. Persistent calcification, significant deformity and/or secondary cranial complications may be an indication for surgical excision. 4,8,9 Treatment of CC is still controversial due to the possibility of a benign clinical course. In neonates, the approach is usually conservative, because the cephalohematoma can be gradually absorbed as the skull develops. Some authors recommend an aspiration attempt for any significantly sized cephalohematoma that fail to reabsorb after a month.3 However, the benefit of aspiration must be outweighed with the risk of infection.4 A passive cranial moulding helmet therapy as a successful nonsurgical treatment for CC causing cranial asymmetry has also been proposed. Moulding is only effective in partially calcified cephalohematomas and probably would yield poor results in completely CC. Furthermore, while moulding is effective in reshaping the skull, this process may push the inner lamella of the cephalohematoma further into the cranial vault, potentially converting a Type 1 into a Type 2 lesion.3 The risk of recurrence with this treatment is also unknown.
A relatively consensual indication for surgery is the correction of skull asymmetry for cosmetic reasons.3,9 Other indications may be the prevention of brain growth restriction, diagnostic confirmation and treatment of associated craniosynostosis.2,9 While experience with surgical correction of CC is limited, the safety and efficacy of intracranial surgery for correction of skull asymmetry in other conditions such as craniosynostosis in children have been well documented, and therefore surgical correction for large calcified cephalohematomas should be considered.3
CONCLUSION
Even though cephalohematoma is frequently encountered, calcified cephalohematoma is seen only sporadically, and is a rare clinical entity. The history and clinical examination are important in the differential diagnosis and imaging strategy. Radiography and ultrasonography are often the initial screening diagnostic tests, followed by magnetic resonance imaging or computed tomography. Head x-ray features, in this case report, where particularly evocative of the diagnosis.
]]>REFERENCES
Nicholson L. Caput succedaneum and cephalohematoma: the cs that leave bumps on the head. Neonatal Netw. 2007; 26:277-81.
Vigo V, Battaglia DI, Frassanito P, Tamburrini G, Caldarelli M, Massimi L. Calcified cephalohematoma as an unusual cause of EEG anomalies: case report. J Neurosurg Pediatr. 2017; 19:46-50.
Wong CH, Foo CL, Seow WT. Calcified cephalohematoma: classification, indications for surgery and techniques. J Craniofac Surg. 2006; 17:970-9.
Guclu B, Yalcinkaya U, Kazanci B, Adilay U, Ekici MA. Diagnosis and treatment of ossified cephalhematoma. J Craniofac Surg. 2012; 23:e505-7.
Piatt JH, Jr. Sagittal synostosis and ossified scalp hematoma: cause or consequence? J Neurosurg Pediatr. 2010; 6:29-32.
Bansal AG, Rosenberg HK. Sonography of pediatric superficial lumps and bumps: illustrative examples from head to toe. Pediatr Radiol. 2017; 47:1171-83.
Moron FE, Morriss MC, Jones JJ, Hunter JV. Lumps and bumps on the head in children: use of CT and MR imaging in solving the clinical diagnostic dilemma. Radiographics. 2004; 24:1655-74
Liu L, Dong C, Chen L. Surgical Treatment of Ossified cephalohematoma: A Case Report and Review of the Literature. World Neurosurg. 2016; 96:614 e7- e9.
Krishnan P, Karthigeyan M, Salunke P. Ossified Cephalhematoma: An Unusual Cause of Calvarial Mass in Infancy J Pediatr Neurosci. 2017; 12: 6466.
CORRESPONDENCE TO
Maria Adriana Rangel
Department of Pediatrics
Centro Hospitalar de Vila Nova de Gaia e Espinho
Rua Dr. Francisco Sá Carneiro
4400-129 Vila Nova de Gaia
Email: mariaadrianarangel@hotmail.com
Received for publication: 05.09.2017 Accepted in revised form: 08.01.2018
{kind=link}