CASE REPORTS | CASOS CLÍNICOS
Interceptive Treatment of Anterior Crossbite: Case series
Tratamento intercetivo da mordida cruzada anterior: Série de casos
Teresa PinhoI,II,III; Diogo MendesI; Carlos Bellot-ArcisIV
I Department of Pediatric Dentistry and Orthodontics, Instituto Universitário de Ciências Saúde, Cooperativa de Ensino Superior Politécnico e Universitário. 4585-116 Paredes, Portugal. teresa.pinho@iucs.cespu.pt; diogofsousamendes@gmail.com ]]>
II IINFACTS Instituto de Investigação e Formação Avançada em Ciências e Tecnologias da Saúde, Cooperativa de Ensino Superior Politécnico e Universitário. 4585-116 Paredes, Portugal. teresa.pinho@iucs.cespu.pt
ABSTRACT
The aim of this paper was to assess changes of the lower cervical-facial proportion for child patients with anterior crossbites (AXB) in interceptive treatment using composite ramps. Intra-oral and facial lateral profile of seven children (4.59 years old) during interceptive treatment of anterior dental (ADXB), functional (AFXB) and skeletal crossbites (ASXB) were used. For ADXB/AFXB, a composite ramp was used; posterior bite composite or sectional fixed braces were added when necessary. In ASXB a facemask and/or composite ramp and brackets were used.
AXB of all patients was improved. ADXB/AFXB (cases 14) were associated with an increased cervical-facial portion (posterior rotation of the mandible), while ASXB/AFXB (cases 57) were associated with a reduced proportion (anterior mandible rotation). Regardless of AXB type, a ramp composite promoted an increase in the vertical dimension and consequently posterior rotation of the mandible, thus worsening the cervical-facial proportion in ADXB/AFXB and improving it in ASXB/AFXB.
Keywords: Anterior crossbite; Anterior functional crossbite; Early treatment; Interceptive treatment; Skeletal anterior crossbite
O objetivo deste trabalho foi avaliar as alterações na proporção cervical-facial inferior de crianças com mordidas cruzadas anteriores (AXB) antes e depois do tratamento intercetivo usando rampas em resina composta. Foram avaliadas as fotos intra-orais e do perfil lateral facial de sete crianças (4,5-9 anos) com mordida cruzado anterior do tipo dentário (ADXB), funcional (AFXB) e esquelética (ASXB). Para ADXB / AFXB, utilizou-se rampas em compósito; Rampas posteriores e aparelhos fixos seccionais foram também utilizados, quando necessário. Na ASXB, utilizou-se rampa em compósito e/ou máscara facial.
AXB de todos os pacientes foi melhorada. ADXB / AFXB (casos 1-4) foram associados a uma porção cervical-facial inferior aumentada (rotação posterior da mandíbula), enquanto ASXB / AFXB (casos 5-7) foram associados a uma proporção reduzida (rotação da mandíbula anterior). Independentemente do tipo AXB, a rampa em compósito anterior promoveu um aumento na dimensão vertical e consequentemente rotação posterior da mandíbula, agravando a proporção cervical-facial em ADXB / AFXB e melhorando em ASXB / AFXB.
Palavras-chave: Mordida cruzada anterior dentária; Mordida cruzada anterior funcional; Mordida cruzada anterior esquelética; Tratamento intercetivo; Tratamento precoce
INTRODUCTION
The anterior crossbite (AXB) malocclusion is an abnormal buccal-lingual relation that leads to an obvious interference with the function and aesthetics of the patient. AXB can be classified as: Dental (ADXB) with a change in one or more teeth, which constitutes the linguo-version of the upper anterior teeth and a buccal-version of the lower anterior teeth with the correct skeletal maxillomandibular relation.1,2 Functional (AFXB) is caused by a dental interference that forces the anterior movement of the mandible when the maximum intercuspidation (MIC). Skeletal (ASXB) is caused by a disharmony of the maxillomandibular bone growth, with compensation of the incisor teeth. To compensate skeletal dysplasia, the upper incisor teeth are often titled towards the front and lower incisors are titled backwards.2-5 The etiology of AXB may be due to genetic or non-genetic factors.2,6
The purpose of early treatment is to eliminate the etiological factors of malocclusion and prevent the progression of dental, skeletal and functional inharmonious. It is possible to minimize or even eliminate the need for complex treatment during permanent dentition.7 The choice of the best method depends on the number of teeth involved, eruptive phase, characteristics of occlusion, severity and patient compliance.6
The composite ramp is a fast, simple, effective and inexpensive method to treat AXB and it does not cause any discomfort.1 Stability is achieved when the tooth is in the correct position.8,9 This individual plan is to make an incisal extension of three to four millimetre in light-cured composite resin held in the antagonist tooth with an angle of 45 degrees to the long axis of the cross element, allowing disocclusion of the posterior teeth. The correction is achieved within one to two weeks without any damage to the tooth or periodontal tissue.1,10 In some cases, a sectioned appliance with braces can be used in order to improve the inclination of the crossed teeth.
]]> Treatment with face mask is used for ASXB and it may correct an AXB problem within one to three months. However, to improve the skeletal relationship, higher collaboration as well as a longer period of time are necessary.
CASE REPORTS
Intra-oral and lateral profile facial photographs of seven children (4.5 and 9 years old) were used in three distinct periods, namely before treatment (T0), after the AXB correction (T1), and one year after the finalization of the interceptive treatment (T2).
Sagittal and vertical analysis were performed using the intra-oral photographs. Soft tissues in T0, T1 and T2 were analyzed in the lateral facial profile, using the relation of the inferior proportion of the Legans face in order to define the tendency of the aesthetic skeletal relation before the treatment (norm = 1.2). Values higher than 1.2 show a tendency to Class II with posterior mandible rotation/retrusion (relation with ADXB/AFXB) and values lower than 1.2 show a tendency to Class III with anterior mandible rotation (relation with ASXB). In case of ADXB/AFXB the composite ramp was the used therapy. When the overbite was increased, a posterior bite composite was added; when the crossed incisor teeth were uneven, sectional fixed braces to these teeth were added. In case of ASXB a facial mask and/or composite ramp and brackets were used.
A lateral profile teleradiograph was used only in cases when a skeletal altered component was diagnosed.
Clinical Case 1
(figure 1):Seven-year-old male with early mixed dentition stage, ADXB between 2.1 (retro-inclined) and 3.1 (pro-inclined) and dental posterior crossbite (DPXB) between 2.6 and 3.6. Convex facial profile, slightly increased relation between the inferior to facial third and and sub-mandibular distance indicating tendency to Class II, confirmed in the cephalometric analysis (convexity of the point A=4.7; norm=2.0±2.0), Class II alveolar (Distance A-B=7.4; norm=5.0±1.0), with norm-maxilla and retro-mandible.
]]>
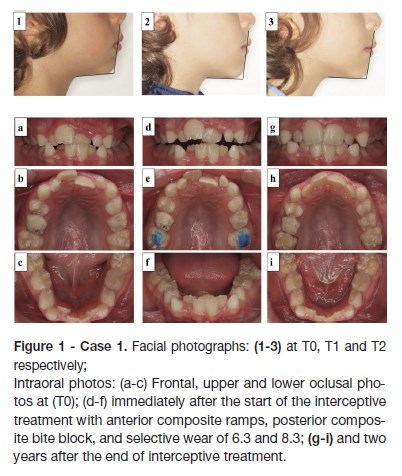
Treatment
A composite ramp (in the lingual face of 3.1 and 4.1), posterior bite composite in the occlusal face of 1.6 and 2.6. A lingual button in the vestibular face of 3.6 and palatine face of 2.6 for crossed elastic was added. Three months after the ADXB and DPXB were corrected. One year after the beginning of the interceptive treatment, the lateral upper incisors teeth were also erupting in crossbite with the primary inferior canines and with a lack of space. Selective wear in occlusal of the 7.3 and 8.3 and in mesial of the 5.3 and 6.3 was immediately applied to facilitate the normalization of the 1.2 and 2.2 in a natural way. The interceptive treatment was completed within three months.
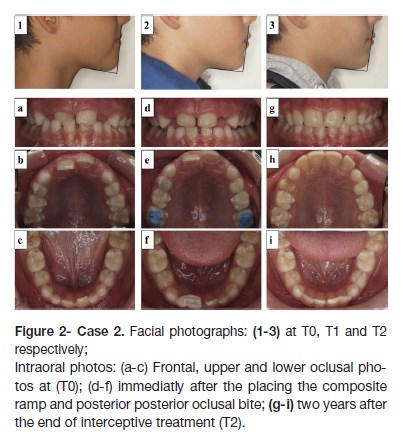
Clinical Case 2
(figure 2): Seven-year-old male with early mixed dentition stage, ADXB in 1.1 with an accentuated negative torque and a high deep-bite. Straight facial lateral profile, increased relation between the inferior third facial and sub-mandibular distance, indicating a Class II tendency.
]]> Treatment
A composite ramp was placed in vestibular and incisal face of 4.1 and posterior bite composite in the occlusal face of 1.6 and 2.6 to allow the stabilization of the occlusion. Due to the accentuated negative torque and high deep-bite in the crossed teeth, two brackets were placed in teeth 1.1 and 2.1 in order to level them (firstly a round arc, followed by a steel rectangular arc and a chain elastic to close the diastema). The interceptive treatment lasted three months.
Clinical Case 3
(figure 3):Sevenyear-old male with mixed dentition stage, total AXB in position of MIC, but with a top-to-top in the CR (considerable functional component). Convex lateral profile, increased relation between the third inferior facial and the sub-mandibular distance of MIC, indicating a Class II tendency. However, when the mandible was manipulated to the CR position, a top-to-top bite in the anterior region was observed, with an improvement in the facial lateral profile. No family member reported relation of skeletal Class III. Teleradiograph in the position of CR with a consequent cefalometric study was made, verifying a skeletal Class III (Convexity of point A=-0.2; norm=2.2±2.2), alveolar Class III (Distance A-B=1.0; norm=5.0±1.0), with tendency to retro-maxilla (SNA=79.9º; norm 82.0º±2.0) and normo-mandibular (SNB=80.0º; norm=80.0º±2.0); upper incisive teeth with buccal-version (UI/NA=27.1º; norm=22º±2), inferior were slightly pro-inclinated (IMPA=92.2; norm=89.5±2.5).
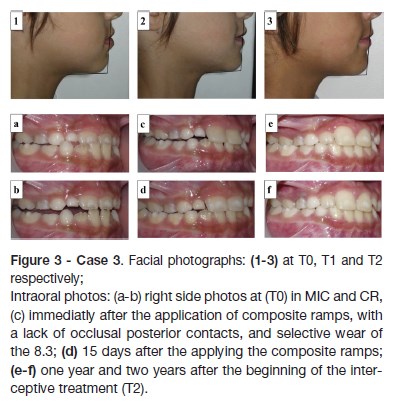
Treatment
Composite ramps in teeth 1.1 and 2.1 were made directly over the vestibular and incisal faces, in order to create a forced positive overjet in CR to pro-incline the upper incisors and retro-inclined the inferior ones. The ramps in composite were removed gradually during the first month when a correction of the AXB was observed with normalized overjet and overbite and occlusal contacts in the posterior region. Two years later, the stability of the results was confirmed.
]]> Clinical Case 4(figure 4): Nine-year-old female with a mixed early dentition, AXB in the central incisors and in the primary canines in the MIC. Despite retro-inclination of upper incisors in the CR, a top-to-top bite was obtained, showing a functional deviation of the mandible. Convex lateral facial profile and an increased relation between the inferior facial third and the sub-mandibular distance in the MIC, indicating a tendency to a Class II. A teleradiograph in the position of MIC was made with a consequent cephalometric study, verifying a skeletal Class I (convexity of the point A=3.0; norm=2.0 ±2.0), alveolar Class II (Distance A-B=8.3; norm=5.0±1.0), with retro-maxilla and retro-mandibulia; upper retro-inclined incisors (UI/MA=14.3º; norm=22º±2) and inferior normoinclined (IMPA=92.5; norm=89.5±2.5).
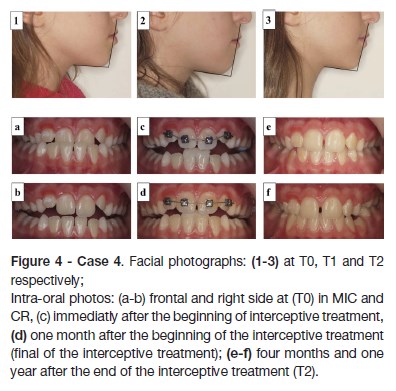
Treatment
A composite ramp in the vestibular and incisal face of 3.1 and 4.1 was made. Due to the highly unevenness of all the upper incisors and the degree of retro-inclination in the central incisors, four brackets were placed in all incisors (1.1, 1.2, 2.1, and 2.2); composite ramp in the 3.1 and 4.1, posterior bite composite in the occlusal face of 1.6 and 2.6 to stabilize of the occlusion. Four months after the crossbite was corrected. One year after, the stability of the results was validated.
Clinical Case 5
(figure 5):Seven-year-old female with mixed dentition, ADXB with retro-inclined central upper incisors, the right one (1.1) more erupted than its contra-lateral (2.1). Straight lateral profile, decreased relation between the inferior facial third and the sub-mandibular distance in the MIC, indicating a tendency to a Class III.
]]>
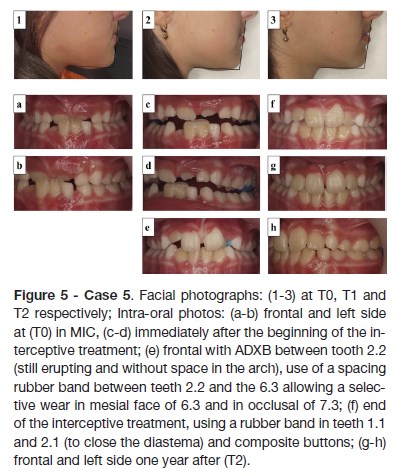
Treatment
A composite ramp in teeth 3.1 and 4.1 (by vestibular and incisal) was added, and posterior occlusal composite was placed in the upper first definitive molars to stabilize the occlusion during the initial stage. Seven days after the ADXB correction between teeth 1.1/4.1 was visible, with a posterior adjustment in tooth 2.1 (that was starting to erupt). One month later the posterior ramps were removed and the anterior ramps were relieved. Two months after the beginning of the treatment, the total correction of the ADXB was observed, so the anterior ramps were removed. Six months later, ADXB between tooth 2.2 (an eruption with a lack of space) and 6.3 was again observed. To correct it, the selective wear in mesial face of 6.3 and an occlusal of 7.3 was used. In order to correct the diastema between the upper central incisors (essentially due to distal inclination of the crown of the 2.1) an elastic (2 oz) was used, with small composite buttons in the vestibular face of the centrals in order to stabilize the elastic (which was changed daily) for the duration of one month. Fifteen months after starting treatment, improvement in the oral condition was indisputable.
Clinical Case 6
(figure 6):Nine-year-old female with mixed dentition. ASXB in 4 upper incisors, bilateral Class III molar and canine. Straight lateral profile, decreased relation between the inferior facial third and sub-mandibular distance in the MIC, indicating a tendency to a Class III. A decreased clinical crown in the first definitive molars was verified, due to the loss of the vertical dimension of the occlusion. Considering the intra and extra-oral characteristics, a telaradiograph in the position of the CR (attachment 5) was made with a consequent cefalometric study. Thus, skeletal Class III (convexity of the point A=-1.3, norm= 2.0±2.0) was concluded, alveolar Class III (Distance A-B=2.8; norm=5.0±1.0), with retro-jaw (SNA=74.4º; norm=82.0±2.0) and retro-mandible (SNB=76.3º, norm=80.0±2.0); upper incisors pro-inclined (UI/NA=32.4º; norm=22º±2) and inferior normo-inclined (IMPA=88.9; norm=89.5±2.5).
]]>
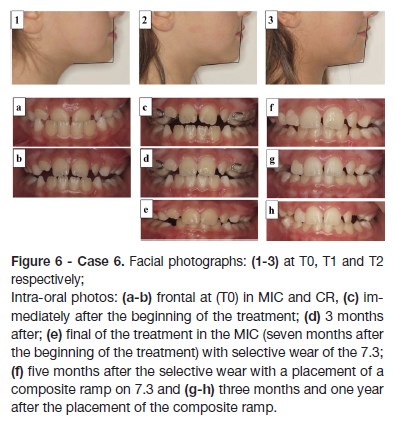
Treatment
A modified MacNamara disjunctor was placed. The acrylic in the first definitive molars was removed in order to allow extrusion. A facial mask was placed at the same time as the expander, so no expansion was needed. Three months later, the inverted bite in the incisors was corrected, with a normal overbite relation. This interceptive treatment lasted six months. After the removal of the disjunctor, inocclusion in the support zone due to the contact of the acrylic and the occlusion of the first molars was observed. A selective wear of the 7.3 was done, considering the forced contact of teeth 2.2 and 7.3 (in crossbite).
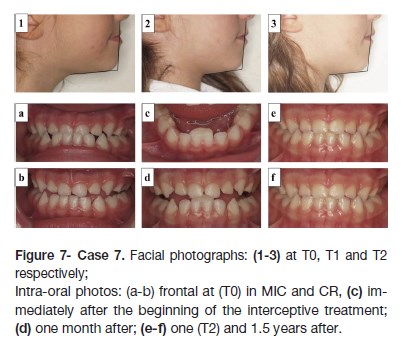
Clinical Case 7
(figure 7): Four-and-half-year old female with primary dentition, ASXB. When the mandible was manipulated to the CR position, a top to top bite in the anterior region was obtained, as such, slight improvement was achieved by using a resin ramp composite. Highlighting the retro-inclination of the lower incisors, a skeletal relation of Class III was conferred. Straight lateral profile, decreased relation between the inferior facial third and the sub-mandibular distance in the MIC, indicated a tendency to the Class III.
]]> Treatment
A composite ramp in teeth 3.1 and 4.1 with some posterior inocclusion was made for the CR position. A month later, the stabilization of the incise position was verified with posterior stable contact. However, ADXB between the 5.2/8.2 and 8.3; 6.2/7.3 teeth was diagnosed. One year later the composite ramp was maintained and kept until the 7.1 and 8.1 root reabsorption.
RESULTS
By analysing the inferior cervico-facial proportion, a tendency to Class II was confirmed in cases 1, 2, 3 and 4, with subsequent rotation/retraction of the mandible (values >1.2). A tendency to Class III (values < 1.2) with anterior rotation of the mandible was diagnosed in cases 5, 6 and 7. In all cases the lower face height increased from T0 to T1/T2.
In all cases the ramp composite was an effective tool to improve the AXB. However, some patients required additional use of occlusal posterior composite (to allow the occlusion stabilization) and/or brackets (to help the proclination of the crossed teeth).
In those with anterior dental crossbite (cases 1 and 2), the occlusion was improved mainly due to the adjustment with torques normalization in the crossed upper incisor teeth that were retro-inclined, associating a facial proportion of Class II tendency (posterior rotation of the mandible).
In the third case, the facial proportions were increased due to lowered submandibular distance caused by posterior rotation of the mandible.
The child with anterior crossbite, as well as functional and dental component (case 4), improved the occlusion due to the correction of upper incisors torque, as well as due to the posterior rotation of the mandible caused by functional component correction.
In the fifth case - anterior crossbite of skeletal type, but with retro-inclination in the upper incisors, lower facial height was increased, thus changing tendency from Class III (anterior mandibular rotation) to Class I.
]]> Orthopedic potentiation of maxillary advancement (using the facemask) helped to improve the facial proportion in case 6, which presented with ASXB pro-inclined upper incisors.In case 7, a child with skeletal and functional crossbites in his primary dentition, the composite ramp was used to enhance the functional component, improving facial proportions until the eruption of permanent teeth.
DISCUSSION
There is limited data in literature evaluating the stability of the correction after the interceptive treatment of the anterior crossbite, whether using the composite ramps or with the facial mask. In addition, no publication that used lateral facial profile repercussions and analyzed the soft tissues before, after the correction of AXB, and at least one year after the treatment (using the relation of the inferior portion of the Legans face to define the tendency of the skeletal relation, as it was done in the present study) was found.
Differential diagnosis has an enormous impact on the determination of the treatment plan, prognosis and stability of the correction. Although the lateral profile teleradiographs are partly the auxiliary means of orthodontics diagnosis, they are only recommended in patients over nine-years-old.11 In the present study, some children were younger than that, thus the profile teleradiographs were performed only in cases which were considered as more serious with possible skeletal component. However, the use of the inferior proportion of the Legans face to define the tendency of the skeletal relation proved to be a suitable diagnosis tool allowing to dismiss cefalometric analysis. The findings reached were consistent in all the cases for which the teleradiographs were made. The ADXB/AFXB cases were associated with an increased cervico-facial proportion (posterior rotation of the mandible), whereas for ASXB/AFXB the proportion decreased (anterior rotation of the mandible). Therefore, a proper treatment plan is fundamental, and above all, to state the correct diagnosis a accurate intra and extra-oral evaluation is necessary.12
After an accurate malocclusion diagnosis it is still necessary to pay attention to certain parameters that influence the correction of AXB. The factors that affect treatment are: the type of anterior crossbite, when it comes to a pseudo Class III, and in most cases realizing that selective wears are a sufficient tool to expedite the correction and help to avoid a relapse, i.e. a good prognosis. However, in the present study cases, the AXB implied the presence of definitive dentition (except for case 7) and therefore the selective wears were not recommended. For this reason, composite ramps were used instead. For those with essential dental type and/or functional type the resolution of the AXB was efficient and fast, mainly due to the retro-inclination of the upper incisor(s). The only case - case 7 witch presented primary dentition, the use of selective wears alone would not have resolved the AXB, not only because of the missing significant functional component but also due to the considerable skeletal alterations, confirmed by a decreased facial proportion. The composite ramp allowed improvement of the functional component. However, due to the skeletal component, parents were warned about the possibility of deterioration when the definitive incisors erupted.
In case of a true Class III malocclusion, that is, the skeletal type, this malocclusion is difficult to treat and contain (an orthopedic treatment is required), therefore it may require a longer-period of treatment.4 As for the sixth case, in order to treat the ASXB, it was necessary to use a disjunction, not to disjunct and expand, but in order to evaluate the bite in the support zone, thus freeing the first definitive molars that were hypo-erupted due to the loss of vertical posterior dimension (VPD). As such, the aim was to allow the unblocking of these first definitive molars and increase the VPD in order to obtain a posterior rotation of the mandible. The facial mask allowed the improvements of the mandible by an orthopedic action and a posterior rotation of the mandible that was helped by the extrusion of the first definitive referred molars. Consequently, the facial proportion was substantially improved, shifting from 1.1 to 1.2 by the end of the treatment and to 1.3 after one year of treatment, improving both dental and facial aesthetics. Before planning a clinical case that involves a high deep bite and AXB, it is expected that it will influence the treatment and retention of the teeth in crossbite.5 In cases 2 and 4, the overbite and the unevenness of the teeth causing AXB led to the use of an occlusal posterior composite in order to create a space for upper incisors so it may vestibularize without occlusal interference with the inferior ones. In some cases, brackets were used in addition to the composite ramp in order to level the upper incisors crowns and to help the vestibularization of teeth in AXB. This support was also needed to improve the significantly altered torque in AXB teeth (strongly retro-inclined).
In some cases, such as in 1 and 5, the posterior composite ramps were needed to stabilize the bite and, therefore, were removed as soon as possible. Once the AXB was corrected, the stabilization and retention depend on the presence of an adequate overbite and the stabilization of the posterior teeth in occlusal contact.1 Therefore, patients who exhibit AXB and little or no overbite are the most difficult cases to treat and contain.5 Sufficient space in the arc is an obvious requirement to correct the AXB so that the respective teeth can move themselves until the desired position in the arc is obtained. If there is insufficient space in the mesio-distal distance of the tooth/teeth in crossbite, the dentist/orthodontist needs to create the necessary space first and only then can they try the uncrossing.5 In first case the lack of space in the arcs was evident; the interproximal wears in teeth adjacent to the AXB (still primary ones) were applied in order to gain the necessary space. In the future, when the respective patient needs a bimaxilar orthodontic treatment, the use of equipment will be minimized. This simplification of the interceptive treatment that causes the antero-inferior alignment must be disregarded, considering that the premature alignment typically complicates the treatment of the AXB.4 The positive root torque in the upper incisors is frequently associated with altered skeletal component of the crossbite, the roots titled towards the palatine and the crown towards the vestibular. In such cases, the use of composite ramps in an isolated form is not advised, because the moment the crown starts to move, uncrossing occurs. Furthermore, in these cases the facial mask is a fundamental orthopedic treatment, improving the skeletal problem and not allowing unnecessary worsening of the pro-inclination of the upper incisors, which is typical in these cases.
It is widely contemplated that the composite ramp is an extreme option, because it works with excessive forces.13 However, it is worth mentioning that periodontal ligament has a proprioceptive refined sensibility, which allows the patient to learn how to quantify the intensity applied to be comfortable and, as such, the tooth in AXB is gradually led to its normal position, inside the physiological threshold.14
]]> There are various procedures reported in literature that can be used for treatment of the AXB.1,4,5,8,9,12-14 However, the composite ramp is a simple procedure, used in the AXB from the dental/functional type, with incredible results obtained within few days.1,15 Still, in all the studied cases independently of the AXB type, treatment with the composite ramp promoted an increase of the VD and consequent posterior rotation of the mandible, thus promoting a worsening /deteoration of the cervivo-facial proportion of ADXB/AFXB and an improvement in the ASXB/AFXB. It should not be forgotten that every case of interceptive treatment is a stressing one, even if shortened, and they require continuous re-evaluations in order to assure that the expected results are being obtained.6When there is an occlusal problem such as the AXB, it is fundamental to highlight the importance of early treatment, immediately after a correct diagnosis, in order to restore the functional equilibrium. Consequently, a balanced and harmonious environment will be provided for a normal maxilo-facial growth.
REFERENCES
1. Pinho T. Mordida cruzada dento-alveolar posterior ou anterior: abordagem simplificada precoce. CiênciaPro 2013; 1:14-23. [ Links ]
2. Lee BD. Correction of crossbite. Dent Clin North Am 1978; 22:647-68. [ Links ]
3. Pinho T. European College of Orthodontics. Commission on Membership and Tenure. Int Orthod 2009; 7:404-14. [ Links ]
]]>4. Pinho T. Prix dexcellence Traitement orthodontico-chirurgical dun cas de Classe III. FBO. Bioprogressive of Orthodontics 2010; 33-42. [ Links ]
5. Costa Pinho TM, Ustrell Torrent JM, Correia Pinto JG. Orthodontic camouflage in the case of a skeletal class III malocclusion. World J Orthod 2004; 5:213-23. [ Links ]
6. Profitt WR, Fields HW, Sarver DM. ContemporaryOrthodontics, 4th ed. St Louis, Elsevier, 2007. [ Links ]
7. Marques LS, Ramos-Jorge ML, Paiva SM, Pordeus IA. Malocclusion: esthetic impact and quality of life among Brazilian schoolchildren. Am J Orthod Dentofacial Orthop 2006, 129:424-7. [ Links ]
8. Croll TP. Correction of anterior tooth crossbite with bonded resin-composite slopes. Quintessence Int 1996; 27:7-10. [ Links ]
]]>9. Estreia FJ, Almerich J, Gascon F. Interceptive correction of anterior crossbite. J Clin Pediatr Dent 1991; 15:157-9. [ Links ]
10. Pinho T. A Ortodontia Intercetiva nas Deformidades Dento-Maxilares. Nascer e Crescer 2011; 20:192-6. [ Links ]
11. Gregoret J. Ortodoncia y Cirugía Ortognática. Diagnóstico yplanificación. 2nd ed, Madrid: NM ediciones, 2007. [ Links ]
12. Seehra J, Fleming PS, Mandall N, Dibiase AT. A comparison of two different techniques for early correction of Class III malocclusion. Angle Orthod 2012; 82:96-101. [ Links ]
13. Santos PCF, Monteiro ALB, Lopes BM, Trévia MC, Chaves AB, Brito DAG. Tratamento Ortodôntico Interceptivo da Mordida Cruzada Anterior: relato de caso clinic, Rev Clín Ortod Dental Press. 2012 11:56-68. [ Links ]
]]>14. Scott C. Orthodontic facemask/protraction face mark used for early treatment of skeletal Class III malocclusion with protraction therapy. J Ir Dent Assoc 2012. 58:64,115. [ Links ]
15. Bayrak S and Tunc ES. Treatment of anterior dental crossbite using bonded resin-composite slopes: case reports. Eur J Dent 2008; 2:303-6. [ Links ]
CORRESPONDENCE TO
Teresa Pinho
Department of Pediatric Dentistry and Orthodontics
Instituto Universitário de Ciências Saúde
Cooperativa de Ensino Superior Politécnico e Universitário ]]>
Received for publication: 11.06.2017
Accepted in revised form: 25.09.2017