QUAL O SEU DIAGNÓSTICO? | WHAT IS YOUR DIAGNOSIS?
Imaging case
Caso imagiológico
Sandra PereiraI; Maria Adriana RangelII; Alexandra MartinsIII; Marta SousaIV; Cristina RochaIII; Arménia OliveiraIII
I Department of Pediatrics, Centro Hospitalar de São João. 4200-319 Porto, Portugal. sandravdpereira@gmail.com ]]>
II Department of Pediatrics, Centro Hospitalar Vila Nova de Gaia/Espinho. 4434-502 Vila Nova de Gaia, Portugal. mariaadrianarangel@hotmail.com
ABSTRACT
Introduction: Congenital Bochdalek Diaphragmatic Hernia (CBDH) is a relatively rare entity and may be underdiagnosed due to not being correctly recognized after the neonatal period.
Case report: An eight-month-old Caucasian infant with failure to thrive, presented to the emergency service with productive cough since the previous week. He was amoxicillin/clavulanic acid prescribed seven days before for an acute otitis media and was afebrile for the past four days. Past history revealed failure to thrive and feeding difficulties. Chest radiograph was misleading, with multiple differential diagnosis, namely eventration and necrotizing pneumonia. Abdominal ultrasonography and thoracoabdominal magnetic resonance imaging revealed CBDH with non-obstructive gastric volvulus.
Discussion: Pediatricians should include late-onset CBDH as a differential diagnosis in any child with recurrent non-specific respiratory or gastrointestinal tract symptoms. Early surgical correction of diaphragmatic defect is crucial to prevent the possible risk of strangulation and severe respiratory problems.
]]> Keywords: Congenital diaphragmatic hernia; cough; failure to thrive; pediatricsRESUMO
Introdução: A Hérnia Diafragmática Congénita de Bochdalek (HDCB) é uma entidade relativamente rara que pode ser subdiagnosticada por não ser corretamente reconhecida após o período neonatal.
Caso Clínico: Criança de oito meses, sexo masculino, caucasiano, recorreu ao Serviço de Urgência por tosse produtiva desde a última semana, sem sinais de dificuldade respiratória. Estava medicado com amoxicilina/ácido clavulânico desde há sete dias por otite média aguda, estando apirético nos últimos quatro dias. Antecedentes de má evolução ponderal e dificuldades alimentares. A radiografia de tórax foi controversa, colocando-se vários diagnósticos diferenciais, como eventração e pneumonia necrotizante. A ecografia abdominal e a ressonância magnética tóraco-abdominal revelaram HDCB com vólvulo gástrico não obstrutivo.
Discussão: Os pediatras devem colocar a HDCB de início tardio como hipótese diagnóstica sempre que uma criança apresente sintomas do aparelho respiratório ou gastrointestinal recorrentes e inespecíficos. A correção cirúrgica precoce do defeito diafragmático é crucial para evitar o potencial risco de estrangulamento ou de problemas respiratórios graves.
Palavras-chave: Hérnia diafragmática congénita; idade pediátrica; má evolução estaturo-ponderal; tosse
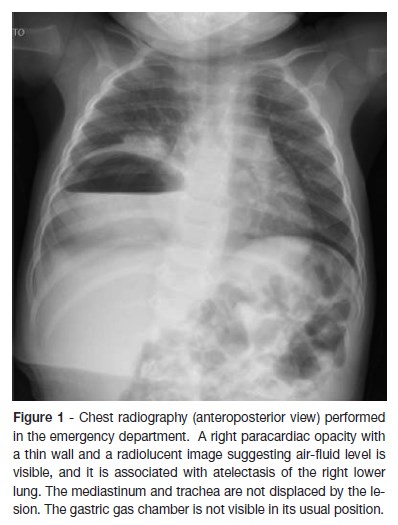
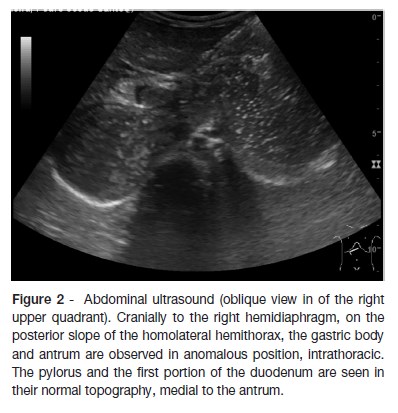
An eight-month-old Caucasian infant, infant presented at the emergency department due to a productive cough starting in the previous week. He was under medication with amoxicillin/clavulanic acid during the past seven days for an acute otitis media and was afebrile three days after beginning of therapy. Past history revealed failure to thrive (crossing percentiles since he was two-month-old: from 50th at birth to below 3rd), without previous etiologic investigation. Food diversification was started at the age of four months and, according to the mother, he was fed in small amounts, more frequently than expected for his age, to avoid vomiting. No other gastrointestinal complaints. On physical examination, he was pale and had an emaciated appearance, without signs of respiratory distress and a normal frequency respiratory rate, with transcutaneous oxygen saturation (SpO2) of 93% at room air. On pulmonary auscultation he had diminished breath sounds in the right pulmonary base, without any adventitious sounds or bulkiness on percussion. Laboratory findings were normal, with negative inflammatory parameters. Chest x-ray (figure 1) detected a paracardiac and right basal nodular shadow with a radiolucent image, as well as a reduction of right lung volume. Differential diagnosis included eventration, congenital diaphragmatic hernia, necrotizing pneumonia, congenital cyst adenomatoid malformation and subphrenic abscess. Abdominal ultrasound (figure 2) showed the gastric body and antrum at an anomalous topography, cranially to the right hemidiaphragm, on the posterior slope of the homolateral hemithorax with associated gastric rotation (non-obstructive volvulus); the pylorus and the first portion of the duodenum were in normal topography. Thoracoabdominopelvic magnetic resonance imaging (figure 3), confirmed the ultrasound findings.
]]>

What is your diagnosis?
DIAGNOSIS
Right-sided Congenital Bochdalek Diaphragmatic Hernia (CBDH)
DISCUSSION
Although the great majority of CBDH are seen in newborns and are unilateral and left-sided, a smaller group of patients present outside neonatal period with an anatomic defect on the right side, as in the case presented. CBDH is the most common embryologic defect of the diaphragm, due to the persistence of the posterolateral pleuroperitoneal canal.1,2 Early-presenting CBDH shows acute symptoms with respiratory compromise after birth, so it is readily diagnosed and requires prompt intervention to prevent death in the neonatal period.1-3 However, a small subset of patients, with a variable prevalence of 2,6-25% off all cases, present this congenital defect beyond this period.1,3-7 Among late-presentation CBDH, unilateral postero-lateral defects constitute more than 96%, with 79,4% and 20,6% left and right-sided hernias, respectively, and is more frequent in males with a ratio of 2:1.1,3,5,6,8 An important epidemiologic feature of late-onset CBHD is a very low incidence of associated anomalies.1,2,5,6 The diagnosis of late-onset congenital diaphragmatic hernia is complicated because it is rare and has a wide spectrum of clinical presentation with inconsistent radiologic findings.1-5,9,10 Presenting symptoms can be both respiratory and gastrointestinal, such as our case, but the later are more common in left-sided CBDH, whereas respiratory symptoms predominate in right-sided hernias.2,5,10 It has been speculated that partial liver herniation, which is a common finding in the right CBHD, may block further herniation of hollow viscera, preventing the development of gastrointestinal symptoms and delaying diagnosis.2,8,10 However, organ herniating into the thorax can cause bilateral mass effects with subsequent respiratory compromise. In our patient, compression of the lung may have led to respiratory symptoms or it may have been a respiratory tract infection that led to the diagnosis while carrying out a chest x-ray. Gastric volvulus led to feeding difficulties and therefore failure to thrive. Cevizci et al reported a case of a 6,5-year-old girl with later presenting CBHD, that was diagnosed in the setting of upper gastrointestinal bleeding due to gastric volvulus with incarceration.1 Malrotation has been found in many patients with late-onset CBDH.5,7 The first-choice technique for assessing diaphragmatic integrity is pulmonary x-ray however it is frequently misdiagnosed.1,3,4,9,10 The most common incorrect radiographic interpretations include pneumonia, congenital cyst adenomatoid malformation, eventration, pneumothorax and pleural effusion, the latter having been associated with inappropriate chest tube insertion with risk of gastrointestinal perforation or bleeding from the thoracic liver.3,4,7-10 Wrong interpretation can be eliminated by inserting a nasogastric tube before scanning.3,8,10 For patients with right CBDH, thoraco-abdominal ultrasound, computerized tomography or magnetic resonance seem to be the best diagnostic option.3,4,8 In this case magnetic resonance imaging findings confirmed Bochdalek hernia and associated gastric volvulus (figure 3). The prompt diagnosis of late-presenting CBDH will reduce morbidity and mortality. Early surgical correction of diaphragmatic defect is crucial to prevent the possible risk of strangulation and severe respiratory problems.3 Therefore, accurate diagnosis and timely minimally invasive surgical intervention ensure an excellent prognosis.3,6-8,10 Our patient underwent laparoscopic surgery, with good clinical evolution.
In summary, late-presenting CBDH should be considered in the differential diagnosis of recurrent non-specific respiratory or gastrointestinal tract symptoms in a child. Although the prognosis associated with late-presenting CBDH is usually favorable, CBDH still requires surgery intervention to alleviate the symptoms and prevent life-threatening complications. Clinicians must maintain a high degree of suspicion for CBDH even beyond the neonatal period, regardless of its presentation, to avoid misdiagnosis, which can result in higher morbidity and mortality. The atypical presentation of this case: failure to thrive in the first months of life and feeding difficulties, and an abnormal chest x-ray, highlights the need of awareness to this condition in order to allow early diagnosis and management.
]]> REFERENCES
1. Cevizci MN, Erdemir G, Cayir A. A Rare Cause of Haemorrhage in the Upper Gastrointestinal System: Bochdalek Hernia. West Indian Med J 2015; 64:154-6. [ Links ]
2. Chang SW, Lee HC, Yeung CY, Chan WT, Hsu CH, Kao HA, et al. A twenty-year review of early and late-presenting congenital Bochdalek diaphragmatic hernia: are they different clinical spectra? Pediatr Neonatol 2010; 51:26-30. [ Links ]
3. Cigdem MK, Onen A, Otcu S, Okur H. Late presentation of bochdalek-type congenital diaphragmatic hernia in children: a 23-year experience at a single center. Surg Today 2007; 37:642-5. [ Links ]
4. Bagłaj M, Dorobisz U. Late-presenting congenital diaphragmatic hernia in children: a literature review. Pediatr Radiol 2005; 35:478-88. [ Links ]
5. Bagłaj M. Late-presenting congenital diaphragmatic hernia in children: a clinical spectrum. Pediatr Surg Int 2004; 20:658-69. [ Links ]
6. Al Ghafri M, Al Sidairi I, Nayar M. Late presentation of congenital diaphragmatic hernia: a case report. Oman Med J 2014; 29:223-5. [ Links ]
7. Mei-Zahav M, Solomon M, Trachsel D, Langer JC. Bochdalek diaphragmatic hernia: not only a neonatal disease. Arch Dis Child 2003; 88:532-5. [ Links ]
8. Radović SV. Late Presentation of Congenital Diaphragmatic Hernia - Case Report. Srp Arh Celok Lek 2015; 143:604-8. [ Links ]
9. Rankin JH, Elkhunovich M, Seif D, Chilstrom M. Point-of-Care Ultrasound Diagnosis of Diaphragmatic Hernia in an Infant With Respiratory Distress. Pediatr Emerg Care 2016; 32:731-3. [ Links ]
10. Kitano Y, Lally KP, Lally PA. Congenital Diaphragmatic Hernia Study Group. Late-presenting congenital diaphragmatic hernia. J Pediatr Surg 2005; 40:1839-43.
]]>CORRESPONDENCE TO
Sandra Pereira
Department of Pediatrics
Centro Hospitalar de São João
Alameda Prof. Hernâni Monteiro
4200319 Porto
Email: sandravdpereira@gmail.com
Received for publication: 13.10.2017
Accepted in revised form: 29.01.2018