Continuous Subcutaneous Insulin Infusion (CSII) Impact on Metabolic Control and Quality of Life of the Informal Caregiver
Perfusão Subcutânea Continua de Insulina (PSCI) - Impacto sobre o Controlo Metabólico e Qualidade de Vida do Cuidador Informal
Maria Adriana RangelI; Carolina BaptistaI; Conceição LimaII; Ana Luísa LeiteII; Rosa Arménia CamposI
I Department of Pediatrics, Centro Hospitalar Vila Nova de Gaia/Espinho. 4400-129 Vila Nova de Gaia, Portugal. mariaadrianarangel@hotmail.com; carolina.baptista@gmail.com
II Unit of Pediatric Endocrinology, Department of Pediatrics, Centro Hospitalar Vila Nova de Gaia/Espinho. 4400-129 Vila Nova de Gaia, Portugal. conceicao2@gmail.com; ana.luisa20@gmail.com; menacampos2@gmail.com
ABSTRACT
Aim: To describe the population of children treated with Continuous Insulin Subcutaneous Infusion (CSII) in a single-center unit and assess the impact on metabolic control. As an additional purpose, we also assessed the perceived burden of the caregivers of children with type 1 diabetes (T1DM) and correlated with the insulin delivery method (CSII vs. multiple daily injections - MDIs).
Methods: Descriptive, cross-sectional, observational study, of all patients with T1DM under CSII treatment, followed in a Pediatric Endocrinology Clinic between January 2011 and September 2016. Outcomes regarding metabolic control were assessed at three points: on initiation of CSII, after three to six months period and at the last appointment. On a second phase of our study, we applied the Informal Caregiver Burden Assessment Questionnaire, drawn and validated for the Portuguese population, to parents of children under CSII and compared them with a sample of parents of children under MDIs.
Results: Of a total of 112 T1DM patients followed, 22 patients under CSII treatment were included, with a mean HbA1c of 7.6 ± 0.9%. CSII use was associated with a reduction on body mass index (BMI) z-score over time, and no differences on HbA1C, blood pressure (BP) and lipid profile. Frequency of severe hypoglycaemia and number of hospitalization for metabolic decompensation were significantly reduced.
A total of 44 caregivers answered the questionnaire, aged between 27-52 years, the majority of the female gender (77.3%). The overall overload perceived was not high (Median [Md]=23.0%; Interquartil range [IQR]: 9.8-35.7). Emotional overload (Md=34.4%), family support (Md=25.0%) and personal life implications (Md=23.9%) were the dimensions that contributed the most to the negative overload felted. When compared between groups (n=20 CSII; n=24 MDIs), there were no differences in total or partial quotation.
Conclusion: CSII was associated with a reduction in BMI z-score, number of severe hypoglycaemia and hospitalization, with no differences in HbA1C, BP or lipid profile. Although many studies indicate an improvement in the quality of life of children with CSII and their caregivers, our study does not point to a reduction in the overload experienced. Addressing caregiver psychological distress and burden, ideally through specific and validated diabetes questionnaires, in family-based treatments such as T1DM are of valuable interest and may improve, overtime, health outcomes.
Key-words: Body mass index; diabetes mellitus type 1; quality of life
RESUMO
]]> Objetivo: Descrever a população de crianças tratadas com dispositivos de Perfusão Subcutânea Contínua de Insulina (PSCI) numa unidade e avaliar o impacto no controle metabólico. Como objetivo adicional, avaliar a sobrecarga sentida pelos cuidadores de crianças com diabetes mellitus tipo 1 (DM1) e correlacionar com o método de administração de insulina (PSCI versus múltiplas injeções diárias - MIDs).Métodos: Estudo descritivo, transversal e observacional, de todos os pacientes com DM1 utilizadores de dispositivos de PSCI, sob acompanhamento na unidade de Endocrinologia Pediátrica entre janeiro de 2011 e setembro de 2016. Os resultados relativos ao controle metabólico foram avaliados em três momentos: no início da PSCI, três a seis meses após e na última consulta. Numa segunda fase do estudo, aplicamos o Questionário da Avaliação da Sobrecarga do Cuidador Informal, desenhado e validado para a população portuguesa, aos pais de crianças sob PSCI e comparamos com uma amostra de pais de crianças com MIDs.
Resultados: De um total de 112 pacientes com DM1 em seguimento na unidade, foram incluídos 22 pacientes com dispositivos de PSCI, cuja HbA1c média era de 7,6 ± 0,9%. O uso de PSCI foi associado a uma redução no z-score do índice de massa corporal (IMC) ao longo do tempo, não se verificando diferenças na HbA1C, pressão arterial (PA) e perfil lipídico. A frequência de hipoglicemias graves e o número de internamentos por descompensação metabólica foram significativamente reduzidas.
Um total de 44 cuidadores responderam ao questionário enviado, com idade entre 27 e 52 anos, a maioria do sexo feminino (77,3%). A sobrecarga global sentida não foi alta (Mediana [Md]=23,0%; amplitude interquartil [AIQ] 9,8-35,7). A sobrecarga emocional (Md=34,4%), o suporte familiar (Md=25,0%) e as implicações na vida pessoal (Md=23,9%) foram as dimensões que mais contribuíram para a sobrecarga negativa sentida. Quando comparado entre grupos (n = 20 PSCI; n = 24 MIDs), não existiram diferenças na cotação total ou parcial.
Conclusão: A PSCI foi associada a uma redução no z-score do IMC, número de hipoglicemias graves e internamentos, sem diferenças na HbA1C, na PA, ou no perfil lipídico. Embora muitos estudos indiquem uma melhoria na qualidade de vida das crianças com PSCI e seus cuidadores, o nosso estudo não aponta para uma redução na sobrecarga sentida. Avaliar o impacto psicológico e a sobrecarga do cuidador, idealmente através de questionários específicos e validados para a diabetes, em tratamentos centrados na família como no caso da DM1, são de particular interesse e podem melhorar, ao longo do tempo, os resultados obtidos.
Palavras-chave: Diabetes mellitus tipo 1; índice de massa corporal; qualidade de vida
INTRODUCTION
Type 1 diabetes (T1DM) accounts for over 90% of childhood and adolescent diabetes. Results from pancreatic β-cell destruction ultimately leading to complete insulin deficiency.1,2 T1DM is one of the most common chronic disease in childhood, with 17.5 new cases per 100.000 children under nineteen years old in Portugal in 2014, and is continually increasing in the last couple of years.3
]]> T1DM diagnosis obliges initiation of lifelong insulin therapy, alongside with frequent blood glucose monitoring (BGM) and healthy lifestyle changes, namely in nutrition management and exercise planning. Intensive therapy leads to better metabolic control and a reduction in insulin requirements. In order to reduce risks of vascular complications, as close to physiological insulin replacement as possible and optimal glycemic control are the current recommendations in all age groups. Continuous subcutaneous insulin infusion (CSII) has proven to be an important ally in the intensive treatment of diabetes.4 It is able to closely simulate the normal pattern of insulin secretion, namely continuous 24-hour basal delivery of insulin upon which are superimposed prandial boluses.5 It has several advantages, particularly useful in young patients, namely:Due to its beneficial effects on glucose control, CSII therapy in T1DM is increasingly used worldwide. 4,5 Accordingly, in Portugal, the number of patients using CSII devices is increasing (2.6 times since 2010), with up to 40% being used by children and adolescents under 18 years old.3 The current recommendations in Portugal are that all children and adolescents eligible with T1DM have, by 2019, access to CSII treatment. 6
Besides its benefits on metabolic control, CSII seems to improve the quality of life (QoL) of children by decreasing the frequency of severe hypoglycaemia, allowing a more flexible lifestyle (namely during exercise time), offering greater sense of control and independence and, hence, higher levels of satisfaction. However, there is discordance between studies in terms of impact on QoL. 5,7,8 Fewer studies, however, analyze the beneficial effect in the QoL of the patient caregiver, but CSII seems to decrease overall parenting stress and fear of hypoglycaemia, lessen problems with nutrition management and improve general well-being. 9,10 Furthermore, there seems to be a positive effect on glycaemic control by decreasing the caregiver psychological distress. 11,12
]]> AIMS
To describe the population of children treated with CSII at a single-center unit and to assess the impact on metabolic control over time. As an additional purpose, and on a second phase of the study, we also assessed the perceived burden of the caregivers of children with T1DM and correlated with the insulin delivery method (CSII vs. MDIs).
METHODS
The study was conducted at a single-center Portuguese Pediatric Endocrinology Clinic, one of the specialized centers providing CSII therapy in Portugal. The records of all patients with T1DM that were users of CSII were retrospectively reviewed with focus on demographic, clinical, and analytical data, between January 2011 and September 2016. Patients were included if age was inferior to 18 years by the time of CSII initiation. Exclusion criteria included follow-up time shorter than three months or discontinuation of CSII therapy and returning to MDIs during follow-up.
We recorded variables in three instants: immediately before initiation of CSII therapy, three to six months after and at the time of the last appointment. The following variables for each patient were recorded: glycated hemoglobin levels (HbA1C), body mass index (BMI) z-scores accordingly to Worlds Health Organization (WHO, 2006), blood pressure (BP) z-scores accordingly to American Heart Association (AHA, 2005), lipid profile, frequency of severe hypoglycaemia and need for hospitalization due to metabolic decompensation in the past year. Severe hypoglycaemia was defined accordingly to International Society for Pediatric and Adolescent Diabetes (ISPAD) as an event associated with severe neuroglycopenia resulting in coma or seizure and/or requiring parenteral therapy (glucagon or intravenous glucose).13 Frequency of hypo and hyperglycaemia, through patients clinical records of BGM, were also collected.
On a second phase of the study, we aimed to assess the burden of the caregiver of the T1DM child and to correlate with the insulin delivery method. A validated questionnaire for the Portuguese population (Informal Caregiver Burden Assessment Questionnaire) was sent electronically to a sample of parents of children on CSII and MDIs from whom e-mail addresses were available, with anonymous and online completion.14 Before filling out the questionnaire, parents answered some demographic questions (such as age, schooling, affiliation) as well as the insulin delivery method. The Informal Caregiver Burden Assessment Questionnaire has 32 questions that weigh seven different dimensions, organized in subscales, namely (1) emotional burden, (2) implications to personal life, (3) financial burden, (4) reactions and requirements, (5) efficacy and control mechanisms, (6) family support, and (7) satisfaction with the role and family. The total and partial quotation of the different subscales were calculated and compared between groups. Primary caregivers were the caregivers who self-identified themselves as primarily responsible for diabetes management.
Statistical analysis was performed using Statistical Package for the Social Sciences® (SPSS IBM®, Statistics Inc., Chicago), 21st version. The Shapiro-Wilk test (p> 0.05) was used to test the normality of the quantitative variables. Values were expressed as percentages for discrete variables, or as mean and standard deviation (SD) for continuous parametric variables. Median (Md) and interquartile ranges (IQR) were used for nonparametric variables. The statistical significance (p<0.05) and the model fit of each independent variable were assessed with de Independent Sample t-test, Paired-sample t-test, Mann-Whitney Test, Fischers exact test and Χ2 analysis.
This study was approved by the ethics committee of our hospital.
]]> RESULTS
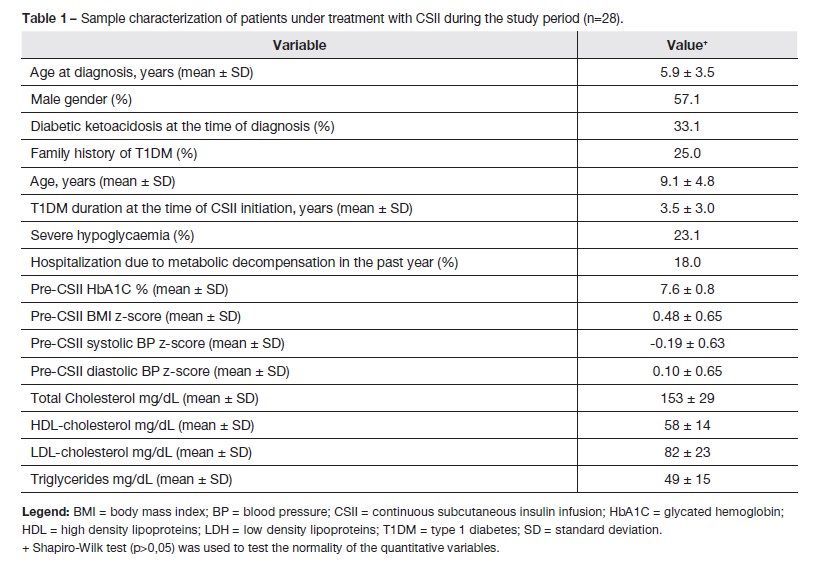
During the study period 28 patients were treated with CSII, which corresponds to 25% of the total sample of T1DM patients followed in the Clinic by that time (n=112). Clinical characteristics of this sample are presented in table 1. Six patients were excluded from the subsequent analysis: four patients because of insufficient time of follow-up and two patients for suspending CSII treatment during follow-up. These two patients were both male adolescents, and acquired CSII device privately instead of the National Health Service. They discontinued after a three years and a five years period on CSII for maladaptation to the system (one following an episode of hyperosmolar hyperglycaemic syndrome due to malfunction of the catheter; the other for reasons of personal incompatibility with physical activity practice).
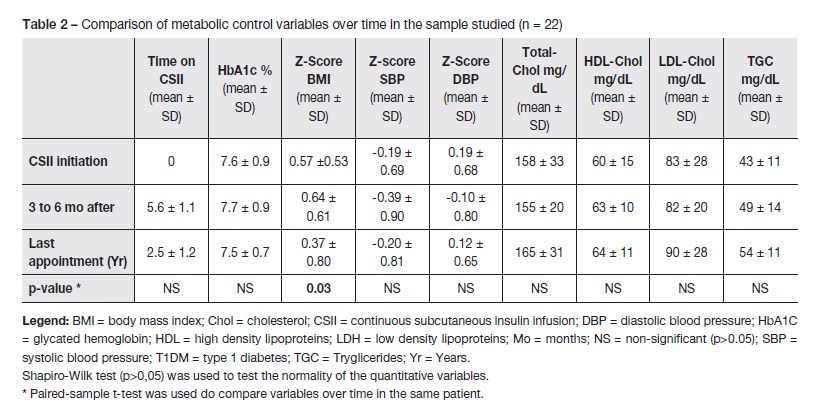
Ultimately, 22 patients were included in the analysis. As seen in table 2, over time there was an improvement in the patient BMI z-score (p=0.03) with CSII treatment. No statistically significant differences were observed in terms of HbA1C, BP and lipid profile. Clinically, there was a reduction in the number of severe hypoglycaemia episodes from 18.2% at the beginning to 0% in the last appointment. The rate of hospitalization also decreased (from 13% before CSII to 0% in the last appointment). In the 3-6 month period post-CSII, there was an increase in the frequency of hyperglycaemia (22.7% to 59.1%) that reduced between that time point and the last appointment (13.5%).
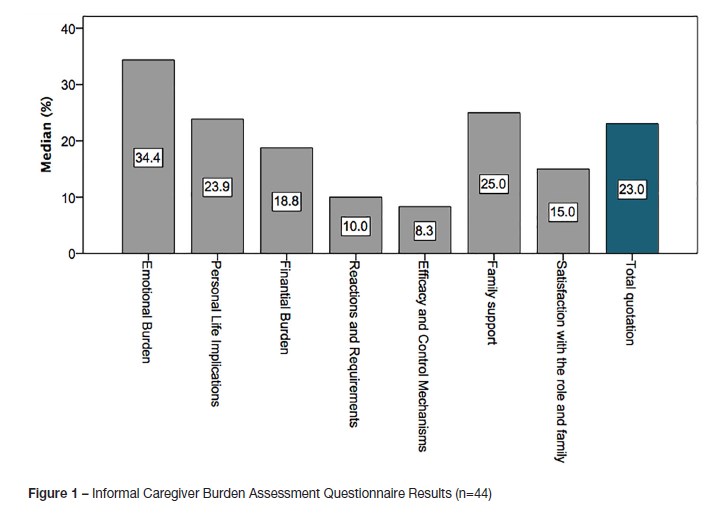
To analyse the physical, emotional and social burden of patients caregiver, 68 Informal Caregiver Burden Assessment Questionnaires were sent electronically. Forty-four parents (65%) consented to participate and returned the questionnaire completed: 20 parents of children on CSII (for a mean of 2.2 ± 2.3 years) and 24 parents of children on MDIs. There was a high degree of internal consistency (ɑ de Cronbach = 0.932). Parents who answered were the main caregivers (77.3%). The majority of them were females (77.3%) and aged between 27 and 52 years (mean 41.8 ± 4.5). The overall overload perceived was 23.0% (IQR: 9.8-35.7). Emotional overload (Md=34.4%; IQR: 12.5-50.0), family support (Md=25.0; IQR: 0.0-50.0) and personal life implications (Md=23.9; IQR: 6.8-39.8) were the dimensions that contributed the most to the negative overload felted (fig. 1). There were no statistically differences (p>0,05) between total or partial quotation and age, gender, schooling, role of primary caregiver, as well as the duration of treatment with CSII.
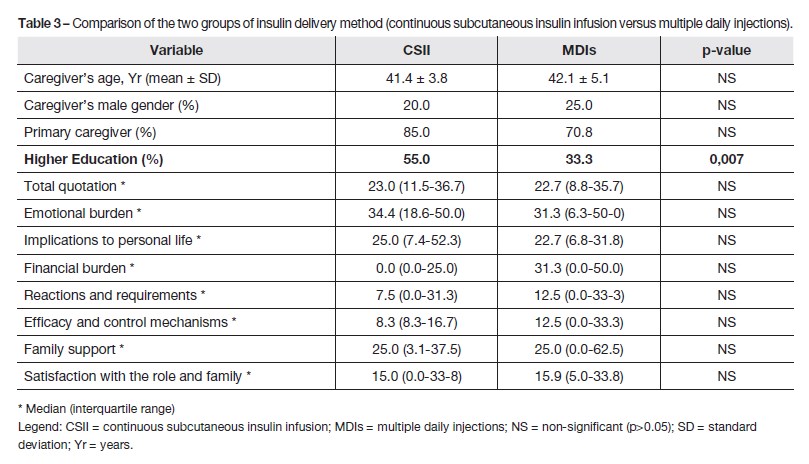
When comparing the two groups (table 3), parents in the CSII group had a higher education level (p<0,01). There were no differences in total or partial quotation on the subscales of the questionnaire.
DISCUSSION
Current literature establishes that CSII attains better glycaemia control, measured by the significant lower level of HbA1C achieved; it also enables a reduction of total daily insulin requirements, a lower BMI z-score, a reduction of severe episodes of hypoglycaemia and ketoacidosis (KA).15-17
Our findings showed a decrease in BMI z-score, and a reduction in the number severe hypoglycaemia and hospitalizations for metabolic decompensation (namely KA episodes). There was no significant reduction in HbA1c. However, this may be the result of a relatively low HbA1c ad initium (7.6 ± 0.9%). HbA1c remained at nearly adequate levels (7.5 ± 0.7%) at 2.5 ± 1.2 years of follow-up. Fear of hypoglycaemia has been described as an issue that can lead to hypoglycaemia avoidance behaviours by parents which adversely affect glycaemic control. 18 We noted an increase in the frequency of hyperglycaemia (22.7% to 59.1%) in the three to six month period post-CSII, that was overcomed, and even reduced, in the last appointment (13.5%), without jeopardizing HbA1c. This may have resulted from fear of hypoglycaemia, that improved as parents felt more confident and self-assured on CSII therapy, as this system leaves no depot in the subcutaneous tissue, and therefore allows a more predictable insulin effect.10
Overall, in our sample of patients, CSII was generally well accepted - only two patients discontinuing treatment with CSII and returning to MDIs. Also, proved to be an adequate therapy, allowing to maintain adequate glycaemic control (with stable satisfactory values of HbA1C), with reduction on severe hypoglycaemia and rates of hospitalization.
]]> However, optimal management of the child with T1DM requires a holistic approach, considering the overall level of function of the child and family, the nutritional and lifestyle patterns specific to that child, and attention to the overall development stages of childhood and adolescence.2 There is no single insulin regime or meal plan appropriate to every patient. The diabetes care plan should fit whenever possible into the surrounding home and school environments.2 Also, the primary childhood tasks of education, socialization, growth, and maturity should continue unhindered by the extra responsibilities diabetes care entails.2 As healthcare providers, we must understand the impact of diabetes and its treatment on the lives of our patients and their families. From the patient and family perspective, the greatest benefits may lie in outcomes beyond measures of glycemic control, such as QoL, and this may have a strong influence on adherence and metabolic control. 19 Recognizing these vital aspects is necessary if optimal outcomes are to be achieved.Most of the published studies, however, focused on medical outcomes such as HbA1c, hypoglycaemia and acute complications. The psychosocial benefits are not as easily measurable as well defined biomedical parameters and, hence, conflicting evidence regarding the impact of CSII on QoL exist.8,9 Because of differences in the age and maturity of the study subjects as well as various forms of diabetes QoL questionnaires used, the results are difficult to analyze and compare.
In a study by Cunningham NR et al , higher A1C values were associated with more caregiver depressive and anxiety symptoms, with stronger association for depressive symptoms.11 Depressive symptoms may lead the caregiver to feel overburdened, and he/she can subsequently withdraw from diabetes management tasks and supervision; anxious caregivers, on the other hand, may remain involved, but be over-extended. When caregivers feel burned by diabetes management, they may be more inclined to transfer responsibility to the adolescent/child or others (grandparents, school assistants, etc.), or to be a less efficient partner in management. These findings, and others, led to consider how perceived burden impacts glycemic control on T1DM and highlights the importance of addressing this issue as part of the diabetes care plane.12
Overall, CSII appears to improve satisfaction with treatment and the burden perceived.7,15,20,21 CSII use seems to decrease hypoglycaemia-related worries, feeding behavior problems and parenting stress, as well as parents burden.10,20 By allowing a more flexible lifestyle, both children and their parents feel more comfortable in going out (such as dinner, parties) and to participate in activities such as travelling, camping and playing, offering greater sense of control and independence and, hence, higher levels of satisfaction.9,21
It can be more challenging and require certain skills to master the technology, mechanical and operational aspects of the pump, which can increase (at least initially) the stress and burden perceived by the parents.9,22 Despite all these challenges, after an initial learning period, CSII allows greater flexibility and autonomy in the management of diabetes, sometimes reducing parents workload.9
As an additional purpose to our work, we attempted to assess the perceived burden of the caregivers of children with T1DM and to correlate it with the insulin delivery method (CSII vs. MDIs) since we hypothesized that the CSII would reduce the burden of patient caregiver. We applied a validated questionnaire for the Portuguese population (Informal Caregiver Burden Assessment Questionnaire), although not specific for T1DM.14
In our study, the majority of the caregivers who answered the questionnaire were female (34/44) and the main caregiver of the child. This difference is possibly due to reflections of cultural patterns, with the role of women in the family as main or primary caregiver. Parents in the CSII group had a higher education level, and this may result from a selection bias. The overall overload perceived was not high (23.9 ± 15.4%), at least comparing with previous studies applying the same questionnaire.23-25 According to what was expected, emotional overload, family support and personal life implications were the dimensions most contributing to the negative overload felt. The total and partial quotations werent related to age, gender, schooling, role of primary caregiver or duration of treatment with CSII. There were no differences between the treatment groups (CSII vs. MDIs), which emphasizes that the choice of insulin delivery method should be based not only on the one that achieves better glycemic control, but also to which the family and child best adjust - two factors that can themselves reduce the burden of the disease.
Several limitations should be taken in account. We used a convenience sample: caregivers that had provided the e-mail address, which may have introduced a selection bias. Data on burden was obtain mainly on the female gender, which may differ from the male gender in their roles and perceived burden, namely emotional (although we didnt find any statistically significant differences in the total and partial quotations and gender). It will be important to obtain a larger sample of caregivers and their perspectives on distress and burden and explicitly through time (in a prospective manner). Also, it would be interesting to correlate the burden felt to the HbA1c of the patients, as is to be expected that one would affect the other. Although we used a validated questionnaire for the Portuguese population to assess caregivers burden, this is not a specific questionnaire for diabetes care, and can miss some specific concerns in the treatment and management of children with diabetes, especially in younger ones. Additionally, we have limited studies to compare the results obtained. A standard QoL questionnaire should be translated and validated for our population that taking into consideration the disease impact, treatment satisfaction and the parents anxiety level, such as Problem Areas in Diabetes Parent Revised Version (PAID-PR).26
In summary, our study showed that CSII is, as described in the literature, a generally well accepted therapy and allowed to maintain good glycaemic control (as monitored by HbA1c), with improvement in BMI Z-score and reduction of the number of severe hypoglycaemia and hospitalization rates. Addressing caregiver psychological distress and burden, particularly depressive symptoms and concerns about diabetes care, ideally through specific and validated diabetes questionnaires, in family-based treatments such as T1DM are of valuable interest and may improve, overtime, health outcomes.
]]> REFERENCES
1. Craig ME, Jefferies C, Dabelea D, Balde N, Seth A, Donaghue KC, et al. ISPAD Clinical Practice Consensus Guidelines 2014. Definition, epidemiology, and classification of diabetes in children and adolescents. Pediatr Diabetes. 2014; 15 Suppl 20:4-17. [ Links ]
2. Sperling MT, Tamborlane WV, Battelino T, Weinzimer SA, Phillip M. Diabetes mellitus. In: Sperling M, editor. Pediatric Endocrinology. 4th Edition ed. Philadelphia, PA Sauders, Elsevier Inc; 2014. p. 849-93. [ Links ]
3. Sociedade Portuguesa de Diabetologia. Diabetes: Factos e Números O Ano de 2015 − Relatório Anual do Observatório Nacional da Diabetes. Diabetologia SPd; 2016. [ Links ]
4. Danne T, Bangstad HJ, Deeb L, Jarosz-Chobot P, Mungaie L, Saboo B, et al. ISPAD Clinical Practice Consensus Guidelines 2014. Insulin treatment in children and adolescents with diabetes. Pediatr Diabetes. 2014; 15 Suppl 20:115-34. [ Links ]
5. Phillip M, Battelino T, Rodriguez H, Danne T, Kaufman F, European Society for Paediatric E, et al. Use of insulin pump therapy in the pediatric age-group: consensus statement from the European Society for Paediatric Endocrinology, the Lawson Wilkins Pediatric Endocrine Society, and the International Society for Pediatric and Adolescent Diabetes, endorsed by the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2007; 30:1653-62. [ Links ]
6. Saúde GdSdEAed. Despacho nº 13277/2016. Diário da República: Diário da República; 2016. [ Links ]
7. Misso ML, Egberts KJ, Page M, OConnor D, Shaw J. Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus. Cochrane Database Syst Rev. 2010:CD005103. [ Links ]
8. Barnard KD, Lloyd CE, Skinner TC. Systematic literature review: quality of life associated with insulin pump use in Type 1 diabetes. Diabet Med. 2007; 24:607-17. [ Links ]
9. Alsaleh FM, Smith FJ, Thompson R, Al-Saleh MA, Taylor KM. Insulin pump therapy: impact on the lives of children/young people with diabetes mellitus and their parents. Int J Clin Pharm. 2014; 36:1023-30. [ Links ]
10. Muller-Godeffroy E, Treichel S, Wagner VM, German Working Group for Paediatric Pump T. Investigation of quality of life and family burden issues during insulin pump therapy in children with Type 1 diabetes mellitus--a large-scale multicentre pilot study. Diabet Med. 2009; 26:493-501. [ Links ]
11. Cunningham NR, Vesco AT, Dolan LM, Hood KK. From caregiver psychological distress to adolescent glycemic control: the mediating role of perceived burden around diabetes management. J Pediatr Psychol. 2011; 36:196-205. [ Links ]
12. Butler DA, Zuehlke JB, Tovar A, Volkening LK, Anderson BJ, Laffel LM. The impact of modifiable family factors on glycemic control among youth with type 1 diabetes. Pediatr Diabetes. 2008; 9:373-81. [ Links ]
13. Ly TT, Maahs DM, Rewers A, Dunger D, Oduwole A, Jones TW, et al. ISPAD Clinical Practice Consensus Guidelines 2014. Assessment and management of hypoglycemia in children and adolescents with diabetes. Pediatr Diabetes. 2014;15 Suppl 20:180-92. [ Links ]
14. Martins TR, JP; Garrett, C. Estudo de Validação do Questionário de Avaliação da Sobrecarga para Cuidadores Informais. Psicologia, Saúde & Doenças. 2003; 4:131-48. [ Links ]
15. Pankowska E, Blazik M, Dziechciarz P, Szypowska A, Szajewska H. Continuous subcutaneous insulin infusion vs. multiple daily injections in children with type 1 diabetes: a systematic review and meta-analysis of randomized control trials. Pediatr Diabetes. 2009; 10:52-8. [ Links ]
16. Sherr JL, Hermann JM, Campbell F, Foster NC, Hofer SE, Allgrove J, et al. Use of insulin pump therapy in children and adolescents with type 1 diabetes and its impact on metabolic control: comparison of results from three large, transatlantic paediatric registries. Diabetologia. 2016; 59:87-91. [ Links ]
17. Szypowska A, Schwandt A, Svensson J, Shalitin S, Cardona-Hernandez R, Forsander G, et al. Insulin pump therapy in children with type 1 diabetes: analysis of data from the SWEET registry. Pediatr Diabetes. 2016;17 Suppl 23:38-45. [ Links ]
18. Barnard K, Thomas S, Royle P, Noyes K, Waugh N. Fear of hypoglycaemia in parents of young children with type 1 diabetes: a systematic review. BMC Pediatr. 2010; 10:50. [ Links ]
19. Faulkner MS, Clark FS. Quality of life for parents of children and adolescents with type 1 diabetes. Diabetes Educ. 1998; 24:721-7. [ Links ]
20. Lukacs A, Kiss-Toth E, Varga B, Soos A, Takac P, Barkai L. Benefits of continuous subcutaneous insulin infusion on quality of life. Int J Technol Assess Health Care. 2013; 29:48-52. [ Links ]
21. Cherubini V, Gesuita R, Bonfanti R, Franzese A, Frongia AP, Iafusco D, et al. Health-related quality of life and treatment preferences in adolescents with type 1 diabetes. The VIPKIDS study. Acta Diabetol. 2014; 51:43-51. [ Links ]
22. Awadalla AW, Ohaeri JU, Al-Awadi SA, Tawfiq AM. Diabetes mellitus patients family caregivers subjective quality of life. J Natl Med Assoc. 2006; 98:727-36. [ Links ]
23. Castelhano P. A sobrecarga dos pais enquanto cuidadores principais da criança com Espinha Bífida: Escola Superior de Enfermagem de Coimbra; 2012. [ Links ]
24. Rodrigues D. Sobrecarga e Estratégias de Coping em Cuidadores Informais de Idosos dependentes. Instituto Politécnico de Viseu, Escola Superior de Saúde de Viseu. 2012. [ Links ]
25. de Souza LR, Hanus JS, Libera LBD, Silva VM, Mangilli EM, Simões PW, et al. Overload in care, stress and impact on the quality of life of surveyed caregivers assisted in primary care. Cad Saúde Colet. 2015; 23:140-9. [ Links ]
26. Markowitz JT, Volkening LK, Butler DA, Antisdel-Lomaglio J, Anderson BJ, Laffel LM. Re-examining a measure of diabetes-related burden in parents of young people with Type 1 diabetes: the Problem Areas in Diabetes Survey - Parent Revised version (PAID-PR). Diabet Med. 2012; 29:526-30. [ Links ]
Maria Adriana Rangel
Department of Pediatrics
Centro Hospitalar Vila Nova de Gaia/Espinho
Rua Francisco Sá Carneiro, ]]>
Received for publication: 07.10.2017
Accepted in revised form: 08.01.2018
{kind=link}
{kind=link}
{kind=link}
{kind=link}