Caso ortopédico
Orthopedic case
Jorge Abreu FerreiraI; Cristiana MartinsI; Paulo PeixotoII; Filipe DuarteIII; José Samaniego TorresI; Jorge França SantosI
I Department of Pediatrics, Centro Hospitalar de Trás-os-Montes e Alto Douro. 5000-508 Vila Real, Portugal. jorgeabreuferreira@gmail.com; cristianamartins@ymail.com; jossama1@yahoo.es; jmfrancasantos@hotmail.com
II Department of Orthopedics, Centro Hospitalar de Trás-os-Montes e Alto Douro. Unidade Hospitalar de Chaves. 5400-279 Chaves, Portugal. paulojrpeixoto@gmail.com ]]>
ABSTRACT
A previously healthy 12-month-old boy, was observed in the emergency department due to refusal to walk, initially diagnosed as transient synovitis of the hip. After one month, he is again observed due to the persistence of symptoms and fever. On objective examination he presented refusal to walk, reporting no difficulties in crawling. A conventional radiography showed lytic lesion on the medial condyle of the left femur and computed tomography (CT) revealed a probable Brodie abscess. Patient was referred to pediatric orthopedics consultation and then performed a magnetic ressonance that confirmed osteomyelitis with an intraosseous abscess. He was submitted to surgical drainage and four weeks of antibiotic therapy, with no sequelae after one year.
Brodies abscess is a subtype of subacute osteomyelitis characterized by the formation of an intramedullary abscess, predominantly in the long bones. It is difficult to diagnose since the symptoms can be mild, mimicking several malignant or benign conditions. Radiology plays a key role in its identification. The treatment can be medical or medical-surgical, usually with a good prognosis.
Keywords: Brodies abscess; osteomyelitis; transient synovitis of the hip
RESUMO
Criança de 12 meses de idade, sexo masculino, observada no serviço de urgência por recusa da marcha. Inicialmente diagnosticada como sinovite transitória da anca. Reobservada após um mês por manutenção dos sintomas e febre. Ao exame objetivo recusava marcha, mas gatinhava bem. Realizou radiografia que mostrou lesão lítica no côndilo medial do fémur esquerdo e tomografia computorizada, que revelou provável abcesso de Brodie. Transferido para observação por ortopedia pediátrica, realizou ressonância magnética, que confirmou osteomielite com abcesso intraósseo. Submetido a drenagem cirúrgica e quatro semanas de antibioterapia, encontrando-se sem sequelas após um ano.
]]> O abcesso de Brodie é um subtipo de osteomielite subaguda caracterizada pela formação de um abcesso intramedular, predominantemente nos ossos longos. É de difícil diagnóstico, uma vez que a sintomatologia é pouco exuberante, podendo mimetizar algumas condições benignas ou malignas. A imagiologia tem um papel fundamental na sua identificação. O tratamento pode ser médico ou médico-cirúrgico, habitualmente com bom prognóstico.Palavras-chave: Abcesso de Brodie; osteomielite; sinovite transitória da anca
A previously healthy 12-month-old boy was admitted in the emergency department due to refusal to walk and a limp on the left leg with a 5-day evolution. There was no history of fever, trauma or recent infection. On admission, besides the refusal to walk, he crawled well and physical examination was unremarkable. Conventional hip radiography and blood tests were normal. Anti-inflammatory medicines were prescribed and he was discharged with the clinical diagnosis of transient synovitis of the hip. After several observations in the emergency department and a month after the initial complaint, he was once again observed due to the persistence of symptoms and fever.
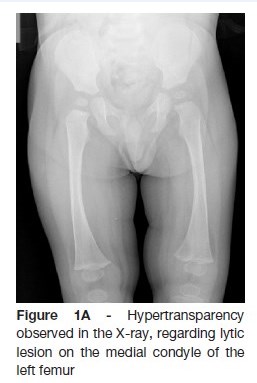
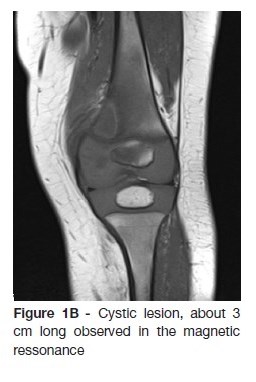
The radiography showed a lytic lesion on the medial femoral condyle (Figure 1A) which was later confirmed by computed tomography and magnetic resonance (Figure 1B).
]]>
What is your diagnosis?
DIAGNOSIS
Brodies abscess
DISCUSSION
]]> Firstly diagnosed by Sir Benjamin Brodie in 1832, Brodies abscess is an uncommon subtype of a subacute osteomyelitis with the formation of an intramedullary abscess. It usually affects the cancellous portion of the metaphyseal, epiphyseal, and diaphyseal long bone and is normally caused by Staphylococcus species.1 The disease has an indolent course due to the combination of host resistance with low virulence of the causative organisms. It is more common in males and usually occurs in young patients.1,2Pain is the most consistent complaint followed by loss of function or limping. Actually, diagnosis is challenging because patients present with mild symptoms and almost normal blood tests.1
Brodies abscess may mimic various benign and malignant conditions such as osteoid osteoma or Ewings sarcoma. Radiology plays an important role in the differential diagnosis, being the magnetic resonance the most commonly used for this purpose.2,3
Biopsy of the Brodies abscess cavity does not usually enable isolation of the microorganism, and therefore it is regarded as non-essential. The initial treatment is primarily conservative, with intravenous antibiotics. Surgical therapy may be an option, in cases of uncertain diagnosis, non-responsiveness to antibiotics, and larger lesions or presenting more aggressive features.1,3
Once the diagnosis is confirmed and the treatment is initiated, results are typically excellent either with medical or medical and surgical treatment.3,4
CASE TREATMENT AND CLINICAL OUTCOME
The patient initiated empirical antibiotic therapy and was referred to a Pediatric Orthopedist specialist. Given the intraosseous abscess size, it was surgically drained. Blood and local exsudate cultures were negative. He completed a two weeks course of intravenous antibiotics (cefuroxime and gentamicin), followed by two weeks of oral antibiotics (cefixime). No sequelae were reported one year after the treatment.
CONCLUSIONS
]]> Although well documented in the literature, Brodies abscess is a rare entity. In this case, normal crawling and hip radiography pointed to an initial misdiagnosis. The authors emphasize the importance of clinical suspicion in a child with refusal to walk, since Brodies abscess can mimic various diseases. Radiology plays a key role in those insidious situations.
REFERENCES
1. Abdulhadi MA, White AM, Pollock AN. Brodie abscess. Pediatr Emerg Care. 2012; 28:1249-51. [ Links ]
2. Agarwal S, Akhtar MN, Bareh J. Brodies abscess of the cuboid in a pediatric male. J Foot Ankle Surg. 2012; 51:258-61. [ Links ]
3. Kornaat PR, Camerlinck M, Vanhoenacker FM, De Praeter G, Kroon HM. Brodies abscess revisited. JBR-BTR. 2010; 93:81-6. [ Links ]
4. Olasinde AA, Oluwadiya KS, Adegbehingbe OO. Treatment of Brodies abscess: excellent results from curettage, bone grafting and antibiotics. Singapore Med J. 2011; 52:436. [ Links ]
CORRESPONDENCE TO
Jorge Abreu Ferreira
Department of Pediatrics,
Centro Hospitalar de Trás-os-Montes e Alto Douro
Av. Noruega, Lordelo
5000-508 Vila Real, Portugal.
Email: jorgeabreuferreira@gmail.com
Received for publication: 21.08.2017 ]]>
Accepted in revised form: 10.01.2018 ]]>