Arthrogryposis multiplex congenita affecting a monochorionic diamniotic twin pregnancy
Artrogripose múltipla congénita em gestação gemelar monocoriónica biamniótica
Rafael BrásI, Helena VelosoI, Maria MoleiroI, Sofia RodriguesI, Gonçalo InocêncioI, Céu MotaII, Gabriela SoaresIII, Maria do Céu RodriguesI, Jorge BragaI
I Obstetrics and Gynecology Department, Centro Materno-Infantil do Norte, Centro Hospitalar Universitário do Porto. 4050-651 Porto, Portugal. rafaelduartebras@gmail.com; h.bragaveloso@gmail.com; lucia.moleiro@gmail.com; sofiapinarodrigues@gmail.com; dr.inocencio@gmail.com; mcpprodrigues@gmail.com; jorgesousabraga@gmail.com
II Pediatrics and Neonatology Department, Centro Materno-Infantil do Norte, Centro Hospitalar Universitário do Porto. 4050-651 Porto, Portugal. ceurmota@gmail.com
III Medical Genetics Department, Centro Hospitalar Universitário do Porto. 4099-001 Porto, Portugal. rafz1@hotmail.com
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
]]> Arthrogryposis multiplex congenita is a clinically and etiologically heterogeneous group of diseases characterized by presence of contractures involving at least two different body areas. It is observed in one in every 3000−5000 live births. A case of singleton arthrogryposis in a spontaneous monochorionic diamniotic twin pregnancy is reported. Diagnosis was established after morphological ultrasound. There were no further complications during pregnancy. After cesarean delivery, diagnosis of amyoplasia involving the four limbs was confirmed. Newborn is currently undergoing motor rehabilitation. The higher risk of singleton arthrogryposis in monochorionic twin pregnancies is documented and appears to be related with vascular changes early in the course of pregnancy. In amyoplasia, some degree of disability and dependency is expected, even with postnatal rehabilitation.Keywords: Amyoplasia; Arthrogryposis; Monochorionic; Twin
RESUMO
A artrogripose múltipla congénita é um grupo clinica e etiologicamente heterogéneo de doenças, caracterizado pela presença de contraturas envolvendo pelo menos duas áreas corporais distintas. Tem uma incidência de 1 em cada 3000−5000 recém-nascidos. É reportado um caso clínico de artrogripose unifetal em gravidez gemelar monocoriónica biamniótica espontânea. O diagnóstico foi estabelecido após ecografia morfológica, tendo a gravidez decorrido sem outras intercorrências. Após parto por cesariana, confirmou-se o diagnóstico de amioplasia envolvendo os quatro membros. O recém-nascido encontra-se atualmente em processo de reabilitação motora. Está documentado o aumento da incidência de artrogripose unifetal na gravidez gemelar monocoriónica, que parece relacionar-se com alterações vasculares na gravidez inicial. Em situações de amioplasia, é de prever a manutenção de algum grau de dependência e incapacidade motora, mesmo com reabilitação pós-natal.
Palavras-chave: Amioplasia; Artrogripose; Gemelar; Monocoriónica
Introduction
Congenital contractures refer to a group of disorders characterized by a decrease in passive/active joint movement amplitude affecting two or more different body areas. They are caused by structural and/or functional anomalies on the surrounding tissues, such as the joint capsule and the periarticular ligaments. In newborns (NBs), incidence of congenital contractures ranges from 1/100 to 1/200, with several possible etiologies and different stages of severity and prognosis.1,2
Arthrogryposis multiplex congenita is a clinically and etiologically heterogeneous group of diseases characterized by the presence of contractures involving at least two distinct body areas. With an incidence of one in every 3000−5000 NBs, it is associated with more than 300 pathologies with a wide range of etiologies.3
]]> The different forms of arthrogryposis can be grouped into six categories concerning etiopathogenesis: (i) myopathic processes (20−30% of cases); (ii) neurologic abnormalities (70−80% of cases); (iii) connective tissue abnormalities; (iv) intrauterine compression; (v) maternal exposure (including to infections as rubella and diseases as diabetes, multiple sclerosis, and myasthenia gravis [the latter of which can cause transient myasthenia of the newborn in about 10% of cases through transplacental passage of antibodies against the recipient, exposure to teratogens, medications, and drugs]); and (vi) vascular compromise of developing fetus, which may explain the high incidence of discordant monozygotic twins.1,3Amyoplasia is the most common form of arthrogryposis and diagnosis is based on clinical findings.
The case of a prenatal diagnosis of arthrogryposis multiplex congenita in one fetus from a monochorionic diamniotic twin pregnancy is presented.
Case report
A 33-year-old pregnant woman, with two miscarriages and one healthy child (G4P1) and diet-managed gestational diabetes reported a spontaneous monochorionic diamniotic twin pregnancy. The couple was non-consanguineous, with no relevant family history.
Patient was referred to the Prenatal Diagnosis Department at 23 weeks of gestation due to detection of joint motion abnormalities on the second fetus in morphological ultrasound evaluation.
First trimester ultrasound was normal, with low combined risk of 21, 18, and 13 trisomies.
Amniocentesis was performed at the local hospital. Chromosome 13, 18, and 21 aneuploidies were excluded. Array-CGH was normal and myotonic dystrophy type one study, negative.
Ultrasound study revealed a monochorionic diamniotic twin pregnancy, with the second fetus presenting a bilateral equinovarus foot, permanently flexed knee joint, permanently extended elbows, and hands in fixed flexion and adduction with permanently flexed fingers (Figure 1). These findings were compatible with the diagnosis of amyoplasia.
]]>

Pregnancy progressed with no further complications.
A cesarean section was performed at 37 weeks, resulting in two live births adequately weighted considering gestational age and Apgar scores of 9/10 for both (Figure 2).
Physical examination of the first fetus was normal.
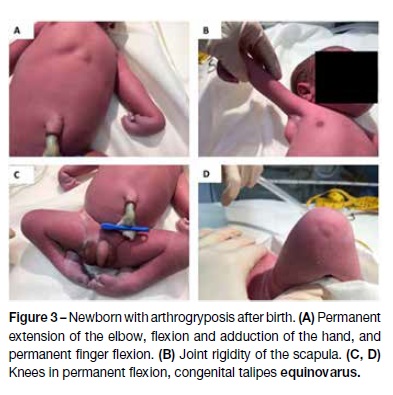
Physical examination of the second fetus confirmed arthrogryposis involving upper and lower limbs. Positional dolichocephaly, slight thoracic asymmetry without intermammary space increase, and absence of lumbar or cervical contractures were reported, with no facial dysmorphia or other physical abnormalities (Figure 3).
]]>
Hospital admission of the newborn at the Neonatal Special Care Unit was uneventful. Physical evaluation revealed no analytical abnormalities and normal transfontanellar and abdominal ultrasounds. Electromyography at the 9th day of life showed signs compatible with acute denervation of distal limb muscles, which were absent from more proximal muscles. Although such signs can be found in cases of non-progressive distal spinal muscular atrophy, a diagnosis of polyneuropathy was less likely due to the normal sensory potential.
Multidisciplinary (Neurology, Medical Genetics, Pediatrics, Orthopedics, Physical Medicine and Rehabilitation) evaluation determined congenital amyoplasia as the most probable diagnosis. Nevertheless, infant’s close follow-up was considered essential, as diagnosis of other rare forms of arthrogryposis was not definitely excluded.
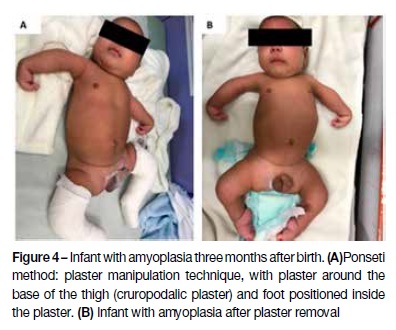
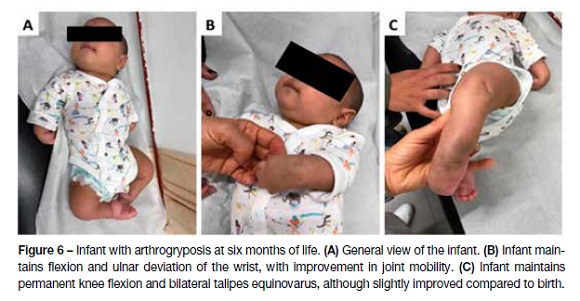
The infant, currently six months old, is undergoing motor rehabilitation with a slight limb mobility improvement (Figure 4, 5, and 6).
]]>
Discussion
According to the literature, detection rate of arthrogryposis in the prenatal period is around 25% 4. In cases of clinical suspicion, either due to decreased fetal movements perceived by the mother or to fetal anatomy anomalies, a thorough echographic evaluation of fetal body movement patterns should be performed. 4
The increased incidence of singleton arthrogryposis in monozygotic twins has been documented, and is thought to be related to vascular changes early in the course of pregnancy.5 Approximately 70% of monozygotic twins are also monochorionic, in which cases an uneven distribution of placental blood circulation may occur.3 When placental blood flow decreases or is disrupted, the developing fetal structures − such as muscles, neuronal structures, and bones - can be easily damaged, with potential impact on fetal development stages. Fetal vascular compromise impairing normal development of nerves or causing death of the anterior horn cells would likely cause fetal neuron, muscle, and bone damage, as well as secondary multiple joint contractures.
Vascular compromise of neuromuscular fetal structures, even transiently, may result in fetal akinesia and joint contractures. Vascular changes are also believed to play a role in the development of abdominal wall defects such as gastroschisis, intestinal atresia, and partial or total absence of finger phalanges.1,5
Amyoplasia is the most common form of arthrogryposis, with an incidence of 1 in 10.000 NB.6 It represents about 30% of all forms of congenital contractures.6 Most cases are sporadic, with etiopathogenesis not fully established. The diagnosis is clinical5 and replacement of normal by fibrous limb muscle tissue and adipocytes is observed.7 Clinically, it is characterized by symmetrical involvement of the four limbs in 60−92% of cases, isolated involvement of lower limbs in 7−24% of cases, and isolated involvement of the upper limbs in 1−13% of cases.1,8
Physical examination of newborns affected with amyoplasia involving the four limbs usually evidences an internal rotation and adduction of the shoulders, extension of the elbows, flexion and ulnar deviation of the wrist, flexion and stiffness of the fingers with adducted thumbs. In the lower limbs, knees appear in flexion or in fixed extension and bilateral equinovarus foot is usually observed. Amyoplasia-affected newborns may also present with dislocated hips.5,9
Patients with amyoplasia have a normal cognitive development.6
Once the diagnosis of amyoplasia is made, rehabilitation should be initiated as soon as possible. Treatment aims to improve quality of life and should engage a multidisciplinary team including pediatrician, orthopedic surgeon, geneticist, physiotherapist, and psychologist. It should be individually planned and include motion rehabilitation of affected joints, active motion restoration in every functional muscle, and correction of fixed deformities affecting daily life activities.6
]]> In 85% of cases, walking can be assured by the age of five.6,9 Success of rehabilitation depends on contracture severity and type of treatment. Pelvic girdle and femoral quadriceps motor capacity play an important role in this process.10Quality of life seems to be mainly determined by motor function of the upper limbs and ability to perform self-care activities.11 Sells et al. demonstrated that around 75% of patients with arthrogryposis are able to self-feed, while only 10% are able to dress unassisted and 35% can perform self-care activities without support.9
If known entities have been excluded, the empiric risk of arthrogryposis recurrence for unaffected parents with an affected child is 3−5%.12
In conclusion, prenatal diagnosis of arthrogryposis is complex. Upon clinical suspicion, a complete evaluation of fetal body movement patterns should be performed. A wide spectrum of conditions can lead to arthrogryposis, and diagnosis of amyoplasia is usually accomplished by excluding other conditions. After delivery, amyoplasia-affected newborn should initiate a complete rehabilitation program. The aim of treatment is to improve quality of life.
REFERENCES
1. Rink BD. Arthrogryposis: a review and approach to prenatal diagnosis. Obstet Gynecol Survey. 2011; 66:369-77. [ Links ]
2. Hall JG. Arthrogryposis multiplex congenita: etiology, genetics, classification, diagnostic approach and general aspects. J Pediatr Orthop B. 1997; 6:159-66. [ Links ]
]]>3. Hall JG. Arthrogryposis (multiple congenital contractures): Diagnostic approach to etiology, classification, genetics, and general principles. European Journal of Medical Genetics. 2014; 57:464-72. [ Links ]
4. Filges I, Hall JG. Failure to identify antenatal multiple congenital contractures and fetal akinesia - proposal of guidelines to improve diagnosis. Prenatal Diagnosis 2013; 33:61-74. [ Links ]
5. Hall JG, Aldinger KA, Tanaka KI. Amyoplasia revisited. American Journal of Medical Genetics Part A. 2014; 164:700-30. [ Links ]
6. Kowalczyk B, Feluś J. Arthrogryposis: An update on clinical aspects, etiology, and treatment strategies. Archives of Medical Science. 2016; 1:10-24.
7. Hall JG, Reed SD, McGillivray BC, Herrmann J, Partington MW, Schinzel A, et al. Part II. Amyoplasia: twinning in amyoplasia - a specific type of arthrogryposis with an apparent excess of discordantly affected identical twins. Am J Med Genet 1983; 15:591-9. [ Links ]
8. Kalampokas E, Kalampokas T, Sofoudis C, Deligeoroglou E, Botsis E. Diagnosing arthrogryposis multiplex congenita: a review. ISRN Obstet Gynecol. 2012; 2012:264918. [ Links ]
9. Sells JM, Jaffe KM, Hall JG. Amyoplasia, the most common type of arthrogryposis: the potential for good outcome. Pediatrics. 1996; 97:225-31. [ Links ]
10. Hoffer M, Swank S, Eastman F, Clark D, Teitge R. Ambulation in severe arthrogryposis. J Pediatr Orthop. 1983; 3:293-7. [ Links ]
11. Fassier A, Wicart P, Dubosset J, Seringe R. Arthrogryposis multiplex congenita. Long term follow up study from birth until skeletal maturity. J Child Orthop. 2009; 3:383-90. [ Links ]
12. Firth HV, Hurst JA. Arthrogryposis (arthrogryposis multiplex congenita). In: Hall JG ed. Oxford Desk Reference Clinical Genetics. 1st ed. Oxford: Oxford University Press; 2005. [ Links ]
]]> Endereço para correspondência | Dirección para correspondencia | Correspondence
Rafael Brás
Obstetrics and Gynecology Department,
Centro Materno-Infantil do Norte
Largo da Maternidade de Júlio Dinis,
4050-651 Porto
Email: rafaelduartebras@gmail.com
Received for publication: 13.09.2017
Accepted in revised form: 05.07.2018
]]>