Bruno Arroja*, Sheila Ferreira**, Manuela Canhoto*, Cláudia Gonçalves*, Filipe Silva*, Isabel Cotrim*, Helena Vasconcelos*, Vítor Pardal***
*Serviço de Gastrenterologia, **Serviço de Medicina Interna 1, ***Serviço de Imagiologia, Hospital de Santo André EPE, Leiria, Portugal
Abstract
Amebiasis is a relatively common infection in developing countries. Entamoeba histolytica is the parasitic agent responsible for invasive forms of this disease.
Abdominal pain and hepatomegaly are classical findings when liver is affected and in some cases large volume abscesses may develop. Despite the mainstay for treatment remains antibiotics, interventional radiology techniques may be useful in more complicated cases.
This report presents a case of invasive amebiasis affecting both the colon and liver of a 75 year old male. Diagnosis, treatment options and follow-up are discussed. The importance of abscess CT guided punction in specific lesions is emphasized.
]]> KEY WORDS: amebiasis, colon, liver, abscess, percutaneous punction.
Amebíase invasiva
Resumo
A amebíase constitui uma forma comum de infecção gastrointestinal nos países subdesenvolvidos, sendo a Entamoeba histolytica o agente parasitário responsável pelas formas invasivas da doença.
A dor abdominal e a hepatomegalia são características clínicas típicas das situações em que se verifica envolvimento hepático, estando descritos na literatura casos de abcessos hepáticos volumosos. Ainda que a antibioterapia seja a base do tratamento, alguns casos mais complexos porém, exigem o recurso a outro tipo de técnicas diferenciadas, nomeadamente as de radiologia interventiva.
Os autores reportam um caso de amebíase invasiva com atingimento intestinal e hepático num homem de 75 anos de idade. São discutidos o diagnóstico diferencial, as opções terapêuticas disponíveis e a evolução da doença.
PALAVRAS-CHAVE: Amebíase, cólon, fígado, abcesso, punção percutânea.
INTRODUCTION
]]> Amebiasis infection is caused in its invasive form by Entamoeba histolyticawhich is a parasite that has an oro-fecal transmission.It is very frequent in tropical areas of the globe, Asia and South America and affects more commonly male patients and children and frequently travellers in these countries1-4. It is also associated with lower socioeconomic classes in endemic areas.1
Intestinal amebiasis is a relatively common cause of dysentery and may present as aqueous/bloody diarrhoea with abdominal cramps and weight loss5. Throughout the colon, amebas can be responsible for the classic flask-shaped ulcers through which the trofozoites gain access to the portal circulation and thereby reach the liver occasionally leading to hepatic abscess formation1-4, 6.
Liver amebiasis is ten times more frequent in males than in women. As much as 80% of all cases present as sub-acute illness. Almost 100% of patients complain of abdominal pain which is usually localized to the right upper abdominal quadrant and is associated with tenderness4, 6-7. Nearly 90% of all liver abscesses are primarily located in the right liver lobe1, 4.
Hepatomegaly is the most important physical finding and fever may not always be present especially in chronic disease.
A proportion of 10-35% of patients with liver amebiasis present with associated gastrointestinal symptoms such as nausea, vomiting, diarrhoea or abdominal pain 3-4.
Laboratory data may reveal mild to moderate leukocytosis and anaemia although severe elevation of white blood count might be found as well as elevated C reactive protein levels. Elevation of alkaline phosphatase and normal alanine aminotransferase are predominant features regarding liver function tests in chronic liver abscess presentation while the inverse relation of these two enzymes is more consistent with acute settings1, 3.
Not infrequently, pulmonary and cardiac complications may emerge in the context of liver abscess secondary to leakage of fluid into the peritoneal cavity or rupture into the pleura or pericardium with consequent possibility of pleural effusion, empyema, atelectasis, pericarditis or tamponade3-4.
Nowadays, intervention radiology techniques are useful in the setting of liver amebiasis once they allow percutaneous drainage of large, life-threatening, or symptomatic lesions8-9.
Typically, the classical “paste of anchovies” fluid is collected from aspirate of liver amebomas3-4, 10.
]]> Although there are multiple diagnostic tools available, it seems that specific serum antigen tests such as ELISA (Enzyme Linked Immuno Sorbent Assay), indirect hemaglutination and indirect immunofluorescence have the highest specificity and sensitivity rates3.Metronidazole plus luminal amebicide remains the mainstay for treating this disease3-4, 10-11.
CASE DESCRIPTION
A 75-year-old Caucasian married male attended the emergency department complaining of postprandial epigastric pain, bloating, vomiting, and hiccups with three hours of onset. Concomitantly he mentioned malaise, anorexia and weight loss for the past month. During the previous week, these symptoms and the abdominal discomfort had become significantly more intense.
He was an active alcoholic drinker with a consumption of approximately 80g per day for nearly thirty years. He regularly travelled to Cape Verde islands in the West African Coast and had made the last trip to this country six months before. Surgeries, blood transfusions, recent sexual misbehaviour or regular chronic medication were denied.
Physical examination revealed a debilitated general appearance. Skin was pale but not jaundiced. Body temperature was 38.0ºC, heart rate 89 bpm, blood pressure 110/75 mmHg; cardiopulmonary auscultation revealed normal cardiac sounds and decreased breath sounds in the lower right third hemithorax; abdomen was distended with tenderness in the right upper abdominal quadrant, hepatomegaly and an irregularly shaped large mass was palpable in the epigastrum.
Laboratory data disclosed: leucocitosys 27.0 x 10^3/ µL, Hb 14.3 g/dL, SR 55%, albumin 20 g/L, BUN 35.9 mg/dL, creatinine 1.2 mg/dL, ALT 82 U/L, AST 103 U/L, total bilirubin 0.9 mg/dL, RCP 329 mg/L.
Thoracic X-ray evidenced elevation of the right hemidiaphragm with ipsilateral pleural effusion (Fig. 1).
]]>

Fig. 1. Thoracic X-Ray showing right pleural effusion and elevation of diaphragmatic cupula.
Ultrasonography showed a single large mass measuring 10 x 12 cm with central necrosis areas in the left liver lobe “suggesting necrotic hepatoma”.
HBV and HCV serologies were negative and alpha-fetoprotein serum level was normal.
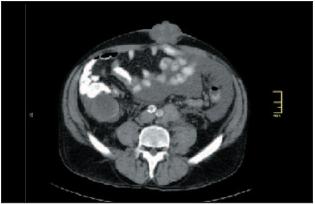
Computed Tomography (CT) scan reported a large heterogeneous lesion with internal septation in the left liver lobe measuring 11 x 8 cm without evident border wall, connecting postero-inferiorly with an extensive liquid and homogenous collection with 16 x 14 cm in diameters which compressed the stomach and nearer viscera (Fig. 2). These radiological findings were confirmed by Magnetic Resonance Imaging. Four days after admission, aqueous diarrhoea with four to five bowel movements per day associated to sustained 38ºC fever ensued.
Fig. 2. CT scan shows a large hepatic abscess.
]]> At colonoscopy, multiple flask-shaped ulcers with congestive mucosa were observed throughout the entire colon (Fig. 3). Biopsies showed ulceration and crypt abscesses but absence of parasites. Neither ova nor parasites were isolated in stool analysis.
Fig. 3. Typical amebiasis colonic flask shaped ulceration.
CT guide aspiration of liver abscess was performed (Fig. 4) allowing drainage of 2500 ml of hematic pus over the following nine days (Fig. 5).

Fig. 4. Liver abscess CT-guided punction.
]]> Antibiotic therapy was started: metronidazole 1g IV bid 10 days plus ceftriaxone 1g IV bid 10 days plus ampicilin 1g IV qid 10 days.
Cultures from blood and abscess aspirate were negative, neither were amebas isolated from pus samples. Significant clinical and laboratorial improvements were seen after few days, whilst diagnosis was confirmed by positive anti-amebiasis ELISA title of 2.4 (positive > 1.1) and positive indirect anti-amebiasis immunofluorescence title of 1/400 (positive 1/100). Serologies for hydatidosis and HIV were negative.
Upon antibiotic treatment, intestinal luminal decontamination was sought with paramomycin 25 mg/kg/day orally for seven days.
Six months follow-up records register an asymptomatic patient with normal weight recovered, normal laboratory data and near normal abdominal features on a CT scan. Colonoscopy reveals mucosal healing in the entire colon.

Fig. 5. Grossly hematic exsudate collected after abscess drainage.
DISCUSSION
The diagnostic path over hepatic amebiasis is not always easy. Differential diagnosis includes pyogenic abscess, necrotic liver tumour and echinococcosis.
]]> The epidemiological context is important but the conjunction of clinical, laboratory and imagiological work may mislead the physicians in the wrong direction as initially happened in this particular case. Development of diarrhoea was a keysymptom which redirected the diagnostic investigation in our case. Initially the possibility of hepatocellular carcinoma seemed consistent as the patient referred weight loss, anorexia, abdominal discomfort and had a past of regular excessive alcohol consumption. In agreement with this hypothesis were an elevated AST/ALT ratio, low serum albumin level and prolongation of prothrombin time. Concomitantly ultrasonography examination was compatible with this hypothesis. The right pleural effusion was at first impression attributed to hypoalbuminemia secondary to liver insufficiency. In fact this is a relatively common pulmonary complication of invasive amebiasis, seen in as much as 20% of all cases4.Percutaneous drainage was performed due to poor clinical improvement secondary to the large lesion size responsible for sustained hiccups and food intolerance in addition to the fact that CT proved rupture of the initial single mass seen on ultrassonographic examination, with formation of a large liquid collection. This procedure is usually safe and yields rapid clinical recovery8-10. Some articles state that although a left sided hepatic lobe collection only happens in 10% of cases, it constitutes an important indication for percutaneous drainage derived from its greater risk of severe complications in case of rupture to near viscera1, 4. The abscess was found to have suffered previous spontaneous rupture so the macroscopic appearance of the collected liquid was purulent-hematic and not the classical “anchovies paste”3-4 that would be to expect.
Since the risk of bacterial infection is enhanced by abscess puncture and colonic mucosa integrity is compromised in invasive amebiasis therefore enabling bacterial translocation, it was decided to start on antibiotics to cover the possibility of a pyogenic abscess.
ELISA assay confirmed the diagnosis as it has almost 100% sensitivity in hepatic amebiasis. It usually remains detectable for the following months. Isolation of amebas in abscess pus or the detection of ova or parasites in stool offers poor outcomes.
Recently a stool antigen test3 has been described with good results but it is yet not generally available. Metronidazole is extremely effective against Entamoeba histolytica since it has rapid intestinal absorption and excellent bioavailability. Despite common side effects such as nausea, metallic taste or headaches, it is a generally well tolerated drug11.
Serious toxic reactions are very rare. It may be administered both orally or intravenously for treatment of hepatic amebiasis12.
Decision to administrate intravenous treatment was due to frequent vomiting and hiccups. In our centre the only available luminal amebicide is paramomycin although agents such aschloroquine, teclosan, ethophamide or nitazoxanide may be helpful if available4. Any of these drugs can be used according to availability, costs and personal experience.
After percutaneous drainage and correct antibiotic treatment, liver healing is achieved in one year in the vast majority of liver amebiasis. Imaging follow up with a CT scan or ultrasonography is advised to confirm improvements.
In conclusion, invasive amebiasis is not always easily manageable and despite being treatable in most cases only with antibiotics, some patients will undergo interventional radiology techniques which seem to be effective and relatively free of complications.
]]> Acronyms
ELISA – Enzyme Linked Immuno Sorbent Assay
bpm – beats per minute
Hb – haemoglobin
PR – prothrombin rate
BUN – blood urea nitrogen
CRP – C Reactive Protein
ALT – Alanine aminotransferase
AST – Aspartate aminotransferase
HBV – Hepatitis B Virus
]]> HCV – Hepatitis C VirusCT – Computed tomography
MRI – Magnetic Resonance Imaging
HIV – Human Immunodeficiency Virus
IV - intravenous
REFERENCES
1 .Shamsuzzaman SM, Haque R, Hasin SK, et al. Socioeconomic status, clinical features, laboratory and parasitological findings of hepatic amebiasis patients – a hospital based prospective study in Bangladesh. Southeast Asian J Trop Med Public Health 2000;31:399-404.
2. Nunes A, Varela MG, Carvalho L, et al. Hepatic amebiasis. Acta Med Port 2000;13:337-343. [ Links ]
3. Haque R, Huston CD, Hughes M, et al. Amebiasis. New Engl J Med 2003;348:1565-1573.
]]> 4. Salles JM, Moraes LA, Salles MC. Hepatic amebiasis. Braz J Infect Dis 2003;7:96-110.5. Salles JM, Salles MJ, Moraes LA, et al. Invasive amebiasis: an update on diagnosis and management. Expert Rev Anti Infect Ther 2007;5:893-901.
6. Berthoud S, Rime F, Buffle P. Amebic liver abscess of unusual presentation. Schweiz Med Wochenschr 1976;12;106:828-830.
7. Chaves FJ, Cruz I, Gomes C, et al. Hepatic amebiasis, analysis of 56 cases. I. Clinical findings. Am J Gastroenterol 1977;68:134-139.
8. Salzano A, Rossi E, Carbone M, et al. Suburban amebiasis: the diagnostic aspects via computed tomography and echography and the percutaneous treatment of amebic liver abscesses. Radiol Med 2000;99:169-173.
9. Avendaño-Arredondo AA, Gil-Galindo G, Garcia-Solis M de J, et al. Clinical experience of early percutaneous drainage of amebic hepatic abscess. Cir Cir 2007;75:157-162.
10. Catalano O, De Rosa A, Cusati B, et al. Diagnostic imaging and interventional radiology of amebic liver abscesses. Personal experience. Radiol Med (Torino) 1999;98:283-287.
11. Gonzales ML, Dans LF, Martinez EG. Antiamoebic drugs for treating amoebic colitis. Cochrane Database Syst Rev 2009;15.
12. Kimura M, Nakamura T, Nawa Y. Experience with intravenous metronidazole to treat moderate-to-severe amebiasis in Japan. Am J Trop Med Hyg 2007;77:381-385.
]]> Correspondência
Bruno Arroja,
Hospital de Santo André EPE, Serviço de Gastrenterologia, Rua das Olhalvas – Pousos
2410–197, Leiria, Portugal;
Contacto telefónico: +351 244 817 000;
Contacto telefónico pessoal: +351 919 917 216
Recebido para Publicação: 01/06/2009 e Aceite para Publicação: 19/08/2010
]]>