A Murinello 1, H Damásio 2, AM Figueiredo 3, J Netta 4, A Carvalho 5, AA Matos 6, MJ Murillo 7 e A Albuquerque 8
1 Graduated Chief Service of Internal Medicine of the HCL (Hospital Curry Cabral)
2 Graduated Hospital Assistant of Internal Medicine (Medicine 1)
3 Resident of Internal Medicine (Medicine 1)
4 Resident of Histopathology
5 Graduated Hospital Assistant of Histopathology
6 Biologist, Ph.D. Superior Technician of Health. Histopathology (Electron Microscopy)
7 Hospital Assistant of Histopathology
]]> 8 Resident of the Common YearUnits: Internal Medicine 1, Histopathology
Hospital Curry Cabral. Lisboa. Portugal
e-mail: amurinello@yahoo.com
Abstract
Based on a case of gastric antral vascular ectasia (watermelon stomach) that was associated with hemorrhagic pericarditis, small cell lung carcinoma with mediastinal lymph node metastases and a synchronous squamous cell carcinoma of the base of the tongue, the authors made a review of the clinical, endoscopic and histopathological aspects of this type of gastropathy, and its association with other diseases, and of the results of its endoscopic therapy. The causes of hemorrhagic pericarditis are considered, emphasizing the necessity to know if the effusion has a malignant etiology. To the best of our knowledge the association of watermelon stomach to small cell lung carcinoma and squamous cell carcinoma of the base of the tongue has not yet been described. Extensive metastases to mediastal lymph nodes are common to small cell lung carcinoma.
Key-words: Gastric antral vascular ectasia, watermelon stomach, small cell lung carcinoma, oat cell lung carcinoma, squamous cell carcinoma of the base of the tongue, hemorrhagic pericarditis.
Estômago em melancia, pericardite hemorrágica, tumor de pequenas células do pulmão e carcinoma pavimentocelular síncrono da base da língua
]]> ResumoBaseados num caso de gastropatia antral com ectasia vascular (estômago em melancia) associado a pericardite hemorrágica e a um carcinoma de pequenas células do pulmão com metástases ganglionares ao longo do mediastino e a um carcinoma pavimentocelular síncrono da base da língua, os autores fazem uma revisão dos aspectos clínicos, endoscópicos e histopatológicos deste tipo de gastropatia, da sua associação a outras doenças e das possibilidades terapêuticas actuais por via endoscópica. Referem-se igualmente as causas mais frequentes de pericardite hemorrágica, salientando-se a origem neoplásica. Não está referida na literatura a associação deste tipo de gastropatia ao carcinoma de pequenas células do pulmão nem ao carcinoma pavimento-celular da base da língua. A invasão extensa dos gânglios mediastínicos pelo carcinoma de pequenas células do pulmão é ocorrência frequente.
Palavras-chave: Gastropatia antral com ectasia vascular, estômago em melancia, carcinoma de pequenas células do pulmão, carcinoma pavimentocelular da base da língua, pericardite hemorrágica.
Introduction
Watermelon stomach is a characteristic endoscopic finding of Gastric Antral Vascular Ectasia (GAVE), so named because of the intensely erythematous longitudinal streaks or columns of ectatic and sacculated blood vessels at the apices of prominent folds running across the gastric antrum and radiating to the pylorus sphincter, and resembling strips on a watermelon rind1,2. GAVE is different from ordinary antral gastritis by its location on the antral folds and sharply demarcated lesion that blanches on pressure3.
GAVE is a rare cause of chronic iron deficiency anaemia due to slow and intermittent gastrointestinal bleeding, brought about by the erosion of submucosal ectatic vessels through the gastric mucosa4. Since the diagnosis is often delayed, it is common for patients to have received multiple packed red cell transfusions5. Even though it is a rare disorder, GAVE is responsible for roughly 4% of non-variceal upper gastrointestinal bleeding6. Profuse gastric hemorrhage is rare with this disorder but may occur as a result of superimposed bleeding diathesis which is present in the majority of patients reporting melena, and is determined by the concomitant presence of conditions such as biliary cirrhosis, valvular heart disease, congestive heart failure, nonsteroidal anti-inflammatory use, CREST syndrome and systemic sclerosis, and chronic renal insufficiency, which can occur in association with watermelon stomach3. Most cases of GAVE are idiopathic and occur more commonly in older women (with a 9:1 female-to-male ratio). Achlorydria is a frequent finding in these patients due to atrophic gastritis7. Rarely, GAVE may occur in association with bone marrow transplantation8, pernicious anemia9, diabetes10, chronic obstructive pulmonary disease10, lymphoma11, glucagonoma12, and neuroendocrine tumor (gastric carcinoid)10.
The association of GAVE with cirrhosis and portal hypertension is considered unreliable with regards to a cause and effect relationship13. It is important to differentiate GAVE from portal gastropathy because the former responds to endoscopic therapy but not to portal hypertension reduction, whereas the latter does not respond to endoscopic therapy but responds to portal pressure reduction13.
The authors present a case of a 59-year-old woman with a previous history of chronic anemia, who was admitted due to acute dyspnea and with an initial diagnosis of hypoxemic bronchopneumonia. The investigation of the patient concludes for the association of GAVE to: (1) Small Cell Lung Carcinoma (SCLC) with mediastinal lymph node metastases, (2) a synchronous Squamous Cell Carcinoma of the base of the tongue, and (3) malignant hemorrhagic pericarditis.
]]> Clinical report
A 59-year-old Caucasian female was admitted to our Unit on 08AUG21 due to progressive dyspnea with a provisory diagnoses of Acute Bronchopneumonia, Congestive Heart Failure and Iron Deficiency Anemia. She was started on Ceftriaxone and Chlarytromycin.
The patient started feeling sick a month prior to admission (PTA), when she became anorexic and asthenic. Fifteen days PTA, the patient developed cough productive of mucopurulent sputum. Ten days PTA, she began to complain of odynophagia and dysphagia for solid food, as well as progressive orthopnea. There was also associated 10 kg weight loss. She denied any other symptoms.Past medical history revealed she had been treated for pulmonary tuberculosis (20 years ago) and gastric ulcer. She was also frequently noted to be anemic. She has been a heavy smoker (40 cigarettes/day) and a heavy alcoholic drinker (but has stopped 12 years ago).
On physical exam she was pale, very thin, profoundly dehydrated, and in respiratory distress with a RR=30 breaths/min, BP=87/68 mm Hg, HR=97 beats/min, T0=35.5ºC. and supraclavicular retraction, blood pressure 87/68 mm Hg, heart rate 97 bpm, temperature 35.5ºC. She was edentulous and had frequent sialorrhoea. There was supraclavicular retraction and numerous supraclavicular lymphadenopathies. Thyroid gland was unenlarged. Auscultation of the lungs revealed bilateral diffuse ronchi and wheezes. Heart sounds were slightly muffled. Negative for breast masses, hepatosplenomegaly and peripheral edema.
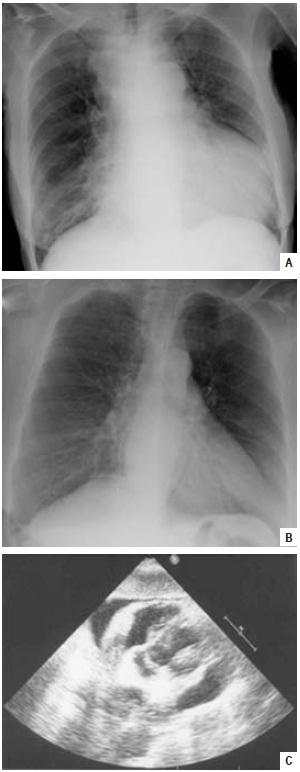
Blood tests showed the following findings: leukocytosis with neutrophilia (18 600/mm3; 94.3%); microcytic anemia (Hb 7.5 g/dL; MCV 76.4 fl; MCH 24.2 pg), adequate platelets. Normal protime, elevated PCR 16.4 mg/dL (N<1.00); hypoalbuminemia 2.62 g/dL; low serum iron and transferrin and ferritin; no monoclonal gammapathy; elevated LDH 752 U/L (N 313-618); other biochemical analysis were normal (glucose; renal and liver function tests; lipid profile; calcium and phosphorus); normal thyroid function tests; Arterial Blood Gas: respiratory alkalosis and hypoxemia (pH 7.514; pCO2 32.7 mmHg; pO2 53.1 mmHg; HCO3 mmol/L; Sat O2 90.2%); several blood cultures, including BACTEC, were negative. Sputum exam: Ziehl-Nielsen and Lowenstein were negative. The Chest PA revealed an enlarged cardiac silhouette, a widened superior mediastinum and an illdefined image of right paracardiac condensation (Fig. 1A). A comparative reading with a chest x-ray dated Dec 2006 (Fig. 1B) lead us to suspect pericardium effusion, which was confirmed by echocardiography, showing massive effusion and signs of cardiac pretamponade, with diastolic collapse of the right atria and pre-collapse of the right ventricle (Fig. 1C), and estimated PSAP of 51 mm Hg. An immediate pericardiocentesis was performed with drainage of 820 mL of pericardial hemorrhagic effusion (in two days) that yielded moderately elevated number of granulocytes and erythrocytes, but negative for Mycobacteria and other bactéria on culture. No malignant cells found. Upper gastrointestinal endoscopy to explain dysphagia showed a normal esophagus, but revealed typical aspects of GAVE (Fig. 2). We were unable to confirm it histologically through biopsy, because the patient became very dyspneic during the procedure. Bronchofibroscopy was not possible to realize due to progressive respiratory failure and the impossibility to do it in our hospital. Biopsy of a supraclavicular lymph node showed infiltration by small cell carcinoma (CAM 5.2 +, AE1/AE3 +, CK7 +; sinaptophysin +, LCA -, TTF1 , cromogranin -; S100 -). The patients condition rapidly deteriorated with development of acute pulmonary edema. After stabilizing the patient, a non-contrast thoracic CT scan (Fig. 3) was done, which revealed prominence of the central pulmonary artery and main right and left branches; numerous hypertrophied mediastinal lymphadenopathies, mainly in the peri-esophageal area, causing compression of the médium esophagus and also of the main right and left bronchus. At the level of right middle lobe and of the lingual lobe there were images suggestive of infection. The patient died on the 7th hospital day (08AUG28) due to respiratory failure. There were no medical conditions to proceed to bronchofibroscopy. Necropsy revealed the following macroscopic and microscopic (hematoxylin-eosin) aspects (Figs. 4 A,B,C; 5 A,B,C; 6 A,B,C; 7 A,B,C): Macroscopically: a) na ulcerated tumor of the base of the tongue measuring 3.5 cm at its widest diameter; b) a mediastinal tumor mass comprising a lymphadenopathic conglomerate involving all the compartments and the right pulmonary hilus, the main right bronchus and a small adjacent area of the lung; c) a tumor metastasis on the right adrenal; d) a tumor metastasis on the right kidney; e) a tumor metastasis on the spleen; Microscopically: a small cell carcinoma (identical to the one described on the ganglionar biopsy) of the right bronchus with extensive mediastinal, tracheal and ganglionar extension, and with metastasis to the spleen, right adrenal, right kidney, pericardium, and hypophysis. Small cell carcinoma was confirmed by neuroendocrine markers using immunohistochemis- try (Fig. 8A). Surprisingly, the tumor located at the tongue base was a (synchronous) squamous cell carcinoma with metastasis only in the hypophysis, which was confirmed by immunohistochemistry (Fig. 8B). There were areas with poorly differentiated pattern but the neuroendocrine markers (sinaptophysin, cromogranin, NSE) were consistently negative. The ultrastructural study performed on both tumors (bronchus and tongue) by electron microscopy confirmed the aforementioned different nature of these tumors (Fig. 9).
Fig. 1 – A/B: PA views of the thorax X-rays (AUG08/DEC06) revealing significant enlarged cardiac silhouette; C: Echocardiography: cardiac pre-tamponade due to voluminous anterior and posterior pericardial effusion
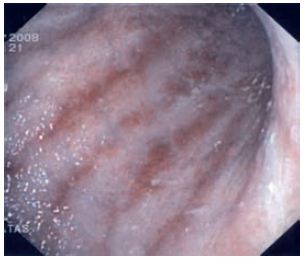
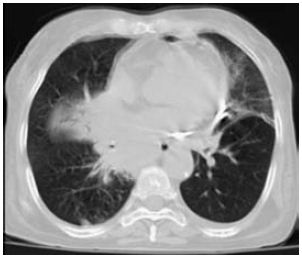
Fig. 3 – Thoracic CT-scan: numerous mediastinic lymphadenopathies causing compression of the medial esophagus and of the main right bronchus
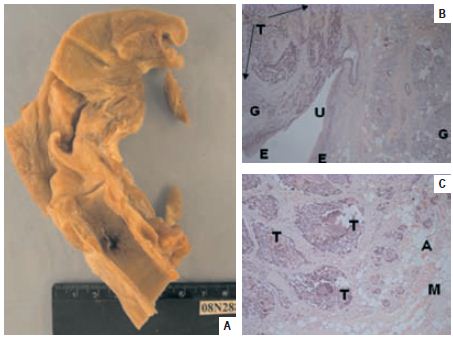
Fig. 4 – A: Base of the tongue with an extensive ulcerated lesion, with macroscopic extension to the valecula; B: HE 10X5 – Squamous neoplasia (T) infiltrating the muscle of the tongue and the minor salivary glands (G), ulcerating (U) the squamous epithelium (E); C: HE 10X10 – Squamous cell carcinoma (T) proliferating and infiltrating the neighbour tissues, adipose tissue (A), muscle (M).
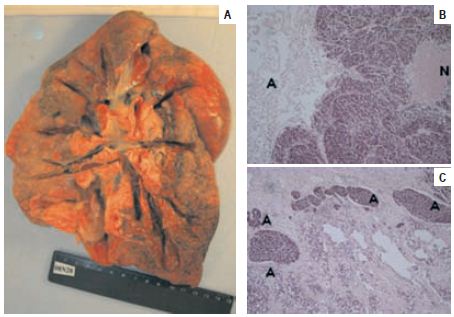
Fig. 5 – A: Right lung with a tumor mass proliferating within the submucosa of the main bronchus and infiltrating the hilus. The mucosal surface of the bronchial tree was intact; B: HE 10X10 – SCLC with necrosis (N); C: HE 10X10 – Lymphatic invasion by the SCLC (A)
]]>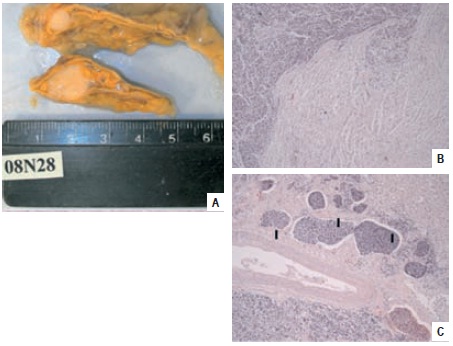
Fig. 6 – A: Macroscopic aspect of adrenal gland metastasis; B: HE 10X10 – Adrenal gland metastasis of SCLC; C: HE 10X10 – Kidney metastasis of SCLC, with lymphatic invasion (I)

Fig. 7 – A: HE 10X10 – Spleen metastasis of SCLC; B: HE 10X10 – Hypophysis gland metastasis of SCLC and squamous cell carcinoma; C: HE 10X10 – Pericardium metastasis of SCLC
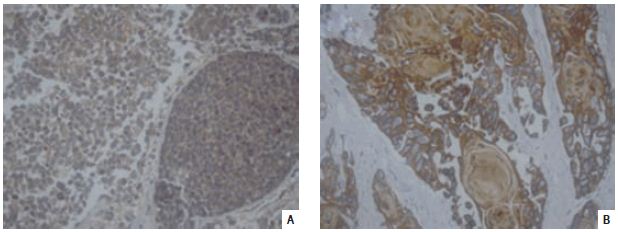
Fig. 8 – Immunohistochemistry: A: 10X40 – SCLC expressing neuroendocrine markers (cromogranin, NSE, and sinaptophysin); B: 10X40 – The neoplasia that involved the hypopharynx, expressed positivity for cytokeratins (34BE12 or CK903)
]]>

Fig. 9 – Post-mortem samples recovered from paraffin blocks and reprocessed for electron microscopy: A: Tumor of the base of the tongue. The cytoplasm of the tumor cells displays well developed bundles of keratin filaments (Q). Inset – High magnification of keratin filament; B: Mediastinic tumor. Dense neurosecretory-like granules (arrows) in the cytoplasm of the tumor cells
Discussion
The findings of a prominent antral folds and antral thickening in upper gastrointestinal radiologic series and on CT scans in na elderly patient with chronic anemia should alert the radiologist to the possibility of GAVE, which should be confirmed endoscopically with biopsy14.
GAVE can be safely biopsied with only minimally increased and minor bleeding because of its low-intravascular pressure. Biopsy of the involved gastric folds reveals characteristic findings of dilated, tortuous mucosal capillaries often occluded by bland fibrin thrombi in the lamina propria and dilated submucosal veins without inflammatory infiltration15,16, together with foveolar hyperplasia and fibromuscular spindle cell hyperplasia of the lamina propria17.
The cause of GAVE is unknown, but Jabbari1 had proposed that it could result from repetitive low-grade trauma caused by repeated prolapse of the loosely attached mucosa of the distal antrum into the duodenum during gastric peristalsis due to antral hypercontractility, primary or acquired, with consequent elongation and secondary reactive muscular hyperplasia and ectasia of the mucosal vessels. Thrombosed ectatic vessels are a distinctive feature and are seen only in GAVE18,19.
Since GAVE is not acid related pharmacotherapy with histamine receptor antagonists and proton pump inhibitors is ineffective. Evidence for effective pharmacologic therapy with oestrogen (and/or progesterone), tranexamic acid or thalidomide, are mentioned in some case reports only6. Ultimately, treatment of any underlying medical comorbidities may lead to resolution of GAVE6. Many authors consider endoscopic therapy as the primary therapy, namely argon plasma coagulation (APC), which appears to be preferable in comparison with contact methods (heater probe, electrocautery with bipolar electrocoagulation probe, or Gold probe) or other noncontact ablative modality (Nd:YAG laser). Despite some contrary opinion10, APC should probably be the treatment of choice for GAVE due to the diffuse nature and superficial location of the lesion20,21. APC is well tolerated and safe because it produces only shallow tissue injury22. Usually several sessions are needed, but requirements of blood transfusions are generally diminished in the large majority of patients23,24,25.
Antrectomy is recommended if endoscopic hemostasis fails. It removes the lesion and nearly always cures the disease, but entails significant morbidity and 5% mortality26.
Despite the generally good results obtained with APC, recently there were some authors who were able to get a much better result with Endoscopic Band Ligation (EBL) in cases of GAVE (especially in patients having large areas of diseased mucosa and submucosa)27 that have been treated with APC but would still have recurrent hemorrhage27. These authors suggest that EBL could be more superior to endoscopic thermal therapy (ETT) for the management of GAVE. In their study consisting of 22 patients treated either with EBL or ETT, including four patients in the EBL group that failed prior ETT, they found that statistically EBL had a significantly higher rate of bleeding cessation (67% vs 23%, P = .04), fewer treatment sessions required for cessation of bleeding (1.9 vs 4.7, P = .05), a greater increase in hemoglobin values ( 2.8 g/dL vs 0.9 g/dL, P = .05), a greater decrease in transfusion requirements ( -12.7 vs -5.2, P = .02), and a greater decrease in hospital admissions ( -2.6 vs -0.5, P = .02) during the follow-up period. EBL for GAVE includes ligation bands applied to abnormal-appearing mucosa in the antrum, beginning in the most distal antrum, adjacent to the pylorus, and subsequently more proximally until as much as possible of the abnormal-appearing mucosa, thus obtaining resection of large amounts of antral mucosa and submucosa. The superiority of EBL compared with ETT is probably due to the fact that EBL providing more reliable obliteration of the abnormal vasculature in the mucosa and submucosa. Complications are also rarer with EBL than with APC27.
]]> The main causes of non-traumatic hemorrhagic pericarditis are tuberculosis in developing countries, frequently associated today with AIDS28, and malignancy in developed29. Meyers et al 30 demonstrated that most pericardial effusions are sero-sanguineous or hemorrhagic (72.6%), there was a great number of possible etiologies, and erythrocytes counts were not significantly different among the diagnostic groups. Other possible causes are post-myocardial infarction rupture of the free wall of the ventricle, retrograde bleeding due to dissecting aneurysm of the proximal thoracic aorta (mostly due to atherosclerotic disease; on old times also syphilitic aneurysm), anticoagulant or antifibrinolytic therapy, congestive heart failure, uremia, connective tissue diseases, and any type of infectious pericarditis31,32,33,34,35,36,37,38,39.In a review of 127 patients with malignancy-related pericardial effusion by Wilkes40, 55% of cases were malignant in etiology while in the remaining 45%, a malignant cause for the effusion could not be determined and no definitive etiology was identified in 74% of these effusions. Diagnosis by cytology and pericardial biopsy had sensitivities of 90% and 50%, respectively. 71% of primary tumors were adenocarcinomas of the lung, breast, esophagus, hematologic malignancies, and of unknown primary site.
Effusions caused by tumors often progress to cardiac tamponade, eliciting bleeding in the pericardium41,42. Malignancy-related hemorrhagic pericardial effusions are frequently a terminal event in patients with disease unresponsive to therapy. However, bloody pericardial effusion can be the presenting manifestation of a newly diagnosed malignancy, either metastatic43,44,45,46,47, or rarely due to primary malignancy of the pericardium (exº mesothelioma48). We shell also think on the possibility of pericardial effusion due to primary malignancy of the heart, and on Kaposi sarcoma and lymphoma in patients with AIDS48.
In most cancer patients with pericardial effusion, or tamponade, it is important that neoplastic involvement of the pericardium be confirmed by identification of malignant cells in pericardial fluid. Confirmation is important because other forms of pericardial disease can occur in patients who have or had cancer48,49,50.
In our patient the cytological examination of the pericardium fluid was negative, but the extensive histological analysis of the pericardium during necropsy, revealed a tiny metastatic focus of small cell carcinoma, confirming the clinical suspicion of a malignant etiology of the pericardium effusion.
The median age at diagnosis for primary cancer of the tongue is 61 years of age. The lifetime risk of developing cancer of the tongue is 1 in 361 men and woman51. People who drink large amounts of alcohol and use tobacco are especially at risk. Tongue cancers are subdivided in cancers of the proximal two-thirds of the tongue buccal tumors, and cancers of the posterior third tongue base cancers or oropharyngeal cancers, which are often diagnosed quite late. Most of the tumors are squamous cells tumors52.
Symptoms of cancer of the tongue are: (a) chronic pain in the pharynx, mostly at mastication or swallowing, (b) numbness of the tongue or of the mouth, (c) a small lump, (d) unexplained bleeding from the tongue53, (e) non-cicatrizing ulcer of the tongue, (f ) otalgia due to pain irradiation, (g) bad breath, (h) drooling, (i) difficulty in breathing, (j) trouble swallowing, (k) difficulty in speaking, (l) bad odour breath. If untreated, the tumor may spread throughout the tongue to the floor of the mouth and to the gum (jaws). As tumor grows it can evolutes to cause metastases to lymph nodes in the neck and later on in the rest of the body54.
Neuroendocrine carcinomas are tumors and are more commonly found in the thyroid, lung and skin. Their diagnosis is based on the recognition of the characteristic morphology and architecture, but immunohistochemical confirmation of the neuroendocrine nature of neoplasm cells is always required.
In our patient, the problem wasnt centered on the histological diagnosis but rather at his origin. The main tumor mass was located at the mediastinum, but is starting to invade the bronchus and lung. We could specu late a thymus origin, but small cell carcinoma is rare at the thymus, and it is much more frequent at the lung. In order to make a diagnosis of small cell carcinoma of the thymus, it is necessary to exclude a lung origin, which we certainly cant do in our case. So, we think that we have to consider that in this patient, the origin was pulmonary with extensive mediastinal and ganglionar extension.
SCLC has an aggressive behavior, with rapid growth, early spread to distant sites (mediastinal lymph nodes, liver, bones, adrenal glands, and brain), frequently exhibit paraneoplasm syndromes and neurologic autoimmune phenomena, and distinct sensitivity to chemotherapy and radiotherapy. Surgery is rarely useful. SCLC generally presents with onset of symptoms within 8-12 weeks prior to admission. The symptoms can result from local tumor growth, intrathoracic spread, distant spread, para-neoplasm syndromes (inappropriate secretion of antidiuretic hormone, ectopic secretion of ACTH) and autoimmune neurologic phenomena. Common symptoms are fatigue, anorexia, weight loss, cough, dyspnea, hemoptysis, symptoms due to vena cava obstruction, hoarseness, dysphagia, stridor, neurological dysfunction, bone pain, abdominal pain due to metastases. Usually SCLC is centrally located and may cause obstruction of the major airway, with distal collapse and post-obstructive pneumonitis. Due to rapid growth and spread, patients at presentation may have a very large intra-thoracic tumor, making difficult to distinguish primary tumor from lymph node metastases. Pleural and pericardial effusions are common55.
]]>Acknowledgments
Due to the following performances at our Hospital: Dr Pratas J (Unit of Gastrenterology) upper gastrointestinal endoscopy; Drs Brizida L and Dr Ramos Aª (Unit of Cardiology) cardiac echocardiography and pericardicentesis; Dr Ramalho V (Unit of Radiology) CT-scan of the thorax
Bibliography
1. Jabbari M, Cherry R, Lough JO, Daly DS, Kinnear DG, Goresky CA. Gastric antral vascular ectasia: the watermelon stomach. Gastroenterol 1984; 87:1165- 1170. [ Links ]
2. Ikeda M, Ishida H, Nakamura E, et al. An endoscopy follow-up study of the development of diffuse antral vascular ectasia. Endoscopy 1996; 28:390-393. [ Links ]
3. Novitsky YW, Kercher KW, Czerniach DR, et al. Watermelon stomach: pathophysiology, diagnosis and management. J Gastroint Surg 2003; 7:652-661. [ Links ]
4. Chatterjee MD. Watermelon stomach. CMAJ 2008; 179:162. [ Links ]
5. Toyota M, Hiroda Y, Nakogawa N. Gastric antral vascular ectasia causing severe anemia. J Gastroenterol 1996; 31:710-713. [ Links ]
6. Selinger CP, Ang YS. Gastric antral vascular ectasia (GAVE): an update on clinical presentation, pathophysiology and treatment. Digestion 2008; 77:131-137. [ Links ]
7. Bersch G. Diffuse gastric antral vascular ectasia: the watermelon stomach revisited (letter). Am J Gastroenterol 1987; 82:1333-1334. [ Links ]
8. Herman BE, Vargo JJ, Baum S, Silverman ED, Eisold J. Gastric antral vascular ectasia: a case report and review of the literature. J Nucl Med 1996; 37:854-856. [ Links ]
9. Gostout CJ, Viggiano TR, Ahlquist DA, Wang KK, Larson MV, Balm R. The clinical and endoscopic Spectrum of the watermelon stomach. J Clin Gastroenterol 1992; 15:256-263. [ Links ]
10. Chaves DM, Sakai P, Oliveira CV, Cheng S, Ishiaka S. Watermelon stomach: clinical aspects and treatment with argon plasma coagulation. Arq Gastroenterol 2006; 43:191-195. [ Links ]
11. Park RH, Danesh BJ, Upadhyay R, Howatson AG, Lec FD, Russel RJ. Gastric antral vascular ectasia (watermelon stomach) therapeutic options. Postgrad Med J 1990: 66:720-723. [ Links ]
12. Weitgasser R, Sungler P, Hauser-Kroberger C, Dietze O, Sattlegger P, Hacker GW. Immunohistochemical assessment of an asymptomatic glucagonoma in a patient with hypergastrinemia and marked antral angiodysplasia. Appl Immunohistochem Molecul Morphol 2001; 9:92-96. [ Links ]
13. Spahr L, Villeneuve JP, Dufresne MP, et al. Gastric antral vascular ectasia in cirrhotic patients: absence of relation with portal hypertension. GUT 1999; 44:739-742. [ Links ]
14. Urban BA, Jones B, Fisman EK, Kern SE, Ravich WJ. Gastric antral vascular ectasia (the watermelon stomach): radiologic findings. Radiology 1991; 178:517-518. [ Links ]
15. Gilliam JH 3rd, Geisinger KR, Wu WC, et al. Endoscopic biopsy is diagnostic in gastric vascular ectasia: the watermelon stomach. Dig Dis Sci 1989; 34:885-888. [ Links ]
16. Cappel MS, Fredal D. Acute nonvariceal upper gastrointestinal bleeding: endoscopic diagnosis and therapy. Med Clin N Am 2008; 92:511-550. [ Links ]
17. Suit PF, Petras RE, Bauer TW, Petrini JL. Gastric antral vascular ectasia: a histologic and morphometric study of the watermelon stomach. Am J Surg Pathol 1987; 11:750-775. [ Links ]
18. DuBouly C, Fairbother J, Isaacson PG. Mucosal prolapse syndrome: a unifying concept for solitary syndrome and related disorders. J Clin Pathol 1983; 36:1264-1268. [ Links ]
19. Tuibia N, Sanyal A. Portal hypertension and variceal hemorrhage. Med Clin N Am 2008; 92:551-574. [ Links ]
20. Pavey DA, Cray PI. Endoscopic therapy for upper GI vascular ectasia. Gastroint Endosc 2004; 59:233-231. [ Links ]
21. Ng I, Lai KC, Ng M. Clinical and histologic features of gastric vascular ectasia: successful treatment with endoscopic laser therapy. J Gastroent Hepatol 1996; 11:270-274. [ Links ]
22. Kwan v, Bourke MJ, Williams SJ, et al. Argon plasma coagulation in the management of symptomatic gastrointestinal vascular lesions: experience in 100 consecutive patients with long-term follow-up. Am J Gastrenterol 2006; 101:58-63. [ Links ]
23. Roman S, Saurin JC, Dumortier J, et al. Tolerance and efficacy of argon plasma coagulation for controlling bleeding in patients with typical and atypical manifestations of watermelon stomach. Endoscopy 2003; 35:1024-1028. [ Links ]
24. Sebastian S, Mehoughin R, Gasim A, et al. Endoscopic argon plasma coagulation for the treatment of gastric antral vascular ectasia (watermelon stomach): longterm results. Dig Liv Dis 2004; 36:212-217. [ Links ]
25. Pereira-Lima JC, Hornos AP, Marques DL, Lopes CV, Waechter FL, Saul C, et al. Tratamento da ectasia vascular do antro gástrico por electrocoagulação com argônio. GED 2002, 21:213-217 (in portuguese). [ Links ]
26. Bourke M, Hope DL, Boyd P, et al. Endoscopic laser therapy for watermelon stomach. J Gastroenterol Hepatol 1996; 11:832-836. [ Links ]
27. Wells CD, Harrison ME, Gurudu SR, Crowell MD, Bynne TJ, Depekis G, et al. Treatment of gastric antral vascular ectasia (watermelon stomach) with endoscopic band ligation. Gastrointest Endosc 2008; 66:231-236. [ Links ]
28. Mayosi BM, Burgess LJ, Douhell AF. Tuberculous pericarditis. Circulation 2005; 112:3608-3616. [ Links ]
29. Dequanter D, Lothaire PH, Berghmans T, Scubier JP. Severe pericardial effusion in patients with concurrent malignancy: a retrospective analysis of prognostic factors influencing survival. Ann Surg Oncol 2008; 15:3268-3271. [ Links ]
30. Meyers DG, Meyers RE, Prendergast TW. The usefullness of diagnostic tests on pericardial fluid. Chest 1997; 111:1213-1221. [ Links ]
31. Hoit BD. Pericardial disease and pericardial tamponade. Crit Care Med 2007; 35:8(Suppl.)S355-S364. [ Links ]
32. Stern JB, Sobel HJ. Hemorrhagic rheumatoid pericarditis. Am J Cardiol 1961; 8: 670-673. [ Links ]
33. Saxena A, Singh N, Romakrishnan S, Kothari S. Bacteriasl pericarditis presenting as hemorrhagic pericardial effusion in a 6-year-old girl. Ann Pediatr Card 2008; 1:68-69. [ Links ]
34. Tenenbaum T, Heusch A, Henrich B, Mackenzie CR, Scmidt KG, Schroten H. Acute hemorrhagic pericarditis in a child with pneumonia due to Chlamydophila pneumonia. J Clin Microbiol 2005; 43:520-522. [ Links ]
35. Zanini G, Antonieli E, Vizzardi E, Raddino R, Cas LD. Hemorrhagic pericarditis with cardiac tamponade due to Coxsackie virus infection. Am J Clin Reports 2008; 9:60-63. [ Links ]
36. Spodick DH. Infectious pericarditis. In Spodick DH (Ed.). The pericardium: a comprehensive textbook. New York: Marcel Dekker 1997: 260-290.
37. Zayas R, Anguit M. Incidence of specific etiology and role of methods for specific etiologic diagnosis of primary acute pericarditis. Am J Cardiol 1995; 75:378- 382. [ Links ]
38. Permaneyer-Miralda G. Acute pericardial disease: approach to the etiologic diagnosis. Heart 2004, 90:252- 254. [ Links ]
39. Olson LJ. Edwards WD, Olney BA, Orsulak TA, Josa M. Hemorrhagic cardiac tamponade: a clinicopathologic correlation. Mayo Clin Proc 1984; 59:785- 790. [ Links ]
40. Wilkes JD, Fidias P, Vaickus L, Perez RP. Malignancy- related pericardial effusion: 127 cases from the Roswell Park cancer Institute. Cancer 1995; 76:1377- 1387. [ Links ]
41. Valley VT, Fly CA. Pericarditis and cardiac tamponade. Available at: http://www.emedicine.com/EMERG/topic412.htm Updated May 12, 2008.
42. Spodik DH. Acute pericarditis, pericardial effusion and cardiac tamponade. Bull Saudy Heart Association 1990; 2:67-76. [ Links ]
43. Atar S, Chiu J, Forrester JS, Siegel RJ. Bloody pericardial effusion in patients with cardiac tamponade Is the cause cancerous, tuberculous, or iatrogenic in the 1990s? Chest 1999; 116:1564-1569. [ Links ]
44. Tsolakis EJ, Charitos CE, Mitsibounas D, Nanas JN. Cardiac tamponade rapidly evolving toward constrictive pericarditis and shock as first manifestation of noncardiac cancer. J Cardiac Surg 2004: 19:134-135. [ Links ]
45. Muir KW, Rodger JC. Cardiac tamponade as the initial manifestation of malignancy: is it as rare as previously supposed? Postgraduate Med J 1994; 70:703- 707. [ Links ]
46. Fincher RM. Case report: malignant pericardial effusion as the initial manifestation of malignancy. Am J Med Sci 1993; 305:106-110. [ Links ]
47. Yuan P-J, Wong W-K. Cardiac tamponade as the initial presentation of thymic carcinoma A case report. Acta Cardiol Sin 2006; 22:112-116. [ Links ]
48. Lewinter MM, Kabbani S. Pericardial diseases. In Zippes DP, Libby P, Bonow RO, Braunwald E (Eds.). Braunwalds heart disease 7th ed. Philadeplia: Elsevier Saunders 2005: 1757-1780.
49. Ben-Horin S, Bank I, Guetta V, Livneh A. Large symptomatic pericardial effusion as the presentation of unrecognized cancer: a study in 173 consecutive patients undergoing pericardiocentesis. Medicine 2996; 85:49-53.
50. Ch iles C, Woodard RD, Singh SP, Lipy GY. Management of pericardial effusion by drainage: a survey of 10 years experience in a city centre general hospital serving a multiracial population. Postgraduate Med J 2000; 76:809-813. [ Links ]
51. Edwards BK (Eds.). SEER cancer statistic reviews, 1997-2005, National Cancer Institute. Bethesda. Available at: http://seer.cancer.gov/csr/1975_2005/.
52. Available at: http://www.mayoclinic.org/tonguebase-cancer/ Tongue base cancer Diagnosis and treatment options at Mayo Clinic.
53. Marioni G, Savartano M, Mattielo L, Koussis H, Carpene S, Marina F, et al. Tongue base metastasis from neuroendocrine endometrial small cell carcinoma. Am J Otolaryng 2007; 28:284-287. [ Links ]
54. Available at: http://www.cancer-info-guide.com/tongue-cancer.html.
55. Magfoor I, Perry M. Lung cancer, oat cell (small cell). In Internet GIST Alliance. Available at: http://emedicine.medscape.com/article/280104, overview, Updated October 15, 2008.
]]>Recebido para publicação/received for publication: 09.05.21
Aceite para publicação/accepted for publication: 10.01.07
]]>