R Duarte 1,2,3,4*, M Villar 5,6* e A Carvalho 1,3*
1 Centro Diagnóstico Pneumológico de Vila Nova de Gaia
2 Centro de Referência de Tuberculose Multi-resistente da Região Norte
3 Centro Hospitalar de Vila Nova de Gaia/Espinho
4 Faculdade de Medicina. Universidade do Porto.
5 Centro Diagnóstico Pneumológico de Venda Nova. Lisboa
6 Centro de Referência Nacional de Tuberculose Multi -resistente
* Comissão de Trabalho de Tuberculose da Sociedade Portuguesa de Pneumologia
]]> Correspondência
Resumo
O diagnóstico e tratamento da infecção latente por Mycobacterium tuberculosis reduz significativamente o risco de desenvolvimento de tuberculose activa e a transmissão da doença na comunidade. O rastreio da tuberculose infecção latente deve passar pela exclusão de doença activa (inquérito de sintomas e radiografia pulmonar) e avaliação da resposta imunológica ao M. tuberculosis através dos testes actualmente ao dispor, como o teste tuberculínico e os testes IGRA (interferon-gamma release assay). A escolha do esquema de tratamento deve ter em linha de conta a eficácia, a adesão e os efeitos colaterais associados ao mesmo Este documento actualiza as recomendações sobre tratamento da tuberculose infecção latente. São apresentadas indicações sobre quem deve ser rastreado e revistos os esquemas de tratamento.
Palavras-chave: Tuberculose, tuberculose infecção latente, tratamento, preventivo.
Latent tuberculosis infection treatment. Current recommendations
Abstract
Diagnosis and treatment of latent infection with Mycobacterium tuberculosis (LTBI), significantly reduces the risk of developing active tuberculosis and the transmission of the disease in the community. LTBI screening must pass by the exclusion of active disease (symptoms enquiry and chest radiography) and assessment of immune response to Mycobacterium tuberculosis testing with the tests currently available tuberculin skin test and interferon-gamma release assay (IGRA). The choice of treatment must take into account the efficacy and side effects associated with the same. This document provides updated recommendations on latent tuberculosis infection treatment. Topics covered include whom to test for TB and reviewed LTBI treatment regimens.
Key words: Tuberculosis, latent tuberculosis infection, treatment, preventive.
]]>Introdução
O tratamento da infecção latente por Mycobacterium tuberculosis reduz significativamente o risco de desenvolvimento de tuberculose activa e a transmissão da doença na comunidade. Assim, o diagnóstico e tratamento da tuberculose infecção latente fazem parte de uma estratégia de eliminação de tuberculose, prevenindo novos casos de tuberculose no futuro1-4. Os estudos de longo prazo foram efectuados com a isoniazida, revelando que a sua administração 3, 6 ou 12 meses, reduzia o risco de evolução para doença em 21%, 65% e 75%, respectivamente5,6. A adesão ao tratamento foi reconhecido como um parâmetro fundamental, sendo a sua eficácia maior quando associada à toma de pelo menos 80% das doses5-9.
Com o objectivo de melhorar a adesão ao tratamento e simultaneamente resolver o problema da infecção com estirpes resistentes à isoniazida, surgiram vários esquemas curtos que são apresentados mais à frente.
O rastreio da tuberculose infecção latente deve passar pela exclusão de doença activa (inquérito de sintomas e radiografia pulmonar) e avaliação da resposta imunológica ao M. tuberculosis através dos testes actualmente ao dispor, como o teste tuberculínico e os testes IGRA (interferon-gamma release assay).
Quem deve ser rastreado para tuberculose infecção latente?
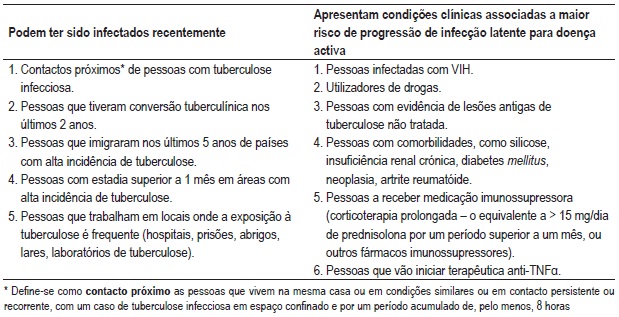
Devem ser rastreados para tuberculose infecção latente todos os indivíduos com risco elevado para tuberculose (Quadro I):
Recentemente infectados e por isso com maior risco de desenvolver doença.
Aqueles que, estando infectados, têm maior risco de desenvolver doença pela coexistência de comorbilidades ou de medicação que interfira com o estado imunitário.
]]> O rastreio de tuberculose infecção latente só deve ter lugar se estiver garantido o tratamento a todas as pessoas identificadas como elegíveis para tratamento. A escolha do esquema de tratamento deve ter em linha de conta a eficácia, a adesão e os efeitos colaterais associados ao mesmo e ser sempre efectuado com o máximo de segurança.
Quadro I Quem deve ser rastreado para tuberculose infecção latente10-15
Esquemas de tratamento
Consideram-se elegíveis para tratamento as pessoas a quem tenha sido efectuado o diagnóstico de tuberculose infecção latente e que pertençam a um grupo de risco acrescido de evolução para tuberculose activa.
Devem ser ponderados os condicionalismos ao tratamento, nomeadamente a coexistência de patologia hepática ou más condições de adesão.
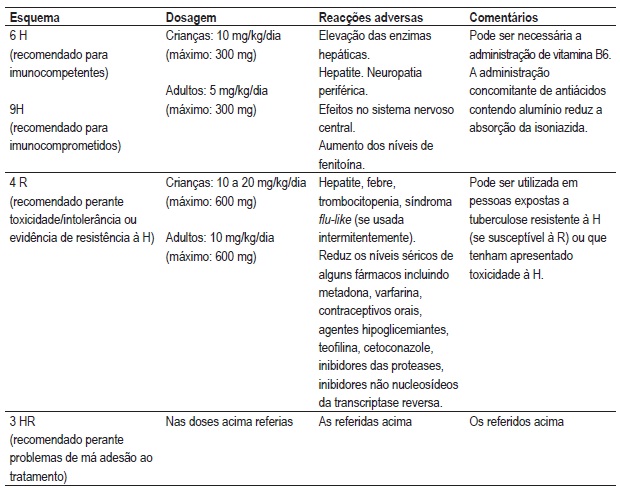
Existem actualmente vários regimes de tratamento da tuberculose infecção latente. Regimes de 6, 9 ou 12 meses de isoniazida (H), de 4 meses de rifampicina (R) ou de 3 meses de isoniazida e rifampicina (HR).
Os regimes contendo rifampicina e pirazinamida deixaram de ser recomendados, devido à sua associação a casos graves de toxicidade hepática, por vezes fatais22,23,24.
Devem ser utilizados esquemas terapêuticos devidamente estudados, com comprovada eficácia e com baixa taxa de efeitos cola terais5,9,10,16-21. No Quadro II, apresentam-se os esquemas terapêuticos que, até à data, cumprem estas características.
]]>Quadro II Esquemas terapêuticos para tratamento da tuberculose infecção latente e efeitos colaterais mais frequentes
Risco de toxicidade medicamentosa
O efeito colateral mais importante é a toxicidade hepática. O risco de toxicidade hepática aumenta com a idade (1,2% no grupo etário dos 35 aos 49 anos e 2,3% dos 50 aos 64 anos) e o consumo de bebidas alcoólicas, ocorrendo na maior parte das situações nos três primeiros meses5,27.
Aqueles que tiverem história de contacto próximo recente ou que têm condições clínicas que aumentem significativamente o risco de progressão para tuberculose activa (infecção por VIH, candidatos a antiTNF alfa) devem ser tratados, independentemente da idade, desde que não apresentem alterações de função hepática antes do início do tratamento.
A administração de vitamina B6 (25 mg/ /dia) reduz os efeitos centrais e periféricos da isoniazida sobre o sistema nervoso central28 e deve ser administrada em pessoas com história de consumo de bebidas alcoólicas, grávidas, mulheres em pós-parto, lactentes, malnutridos, infectados com VIH, pessoas com neoplasia, doença hepática, diabetes ou neuropatia periférica preexistente.
Monitorização
Todos os indivíduos em tratamento para tuberculose infecção latente devem ser monitorizados regularmente. Esta monitorização deve envolver exame clínico, estudo analítico (se necessário) e educação sobre sinais e sintomas de reacções adversas aos fármacos utilizados29.
]]> A avaliação laboratorial inicial deve incluir hemograma e estudo de função hepática e deve ser repetida mensalmente nos indivíduos:
VIH positivos
Com história de consumo de bebidas alcoólicas, doença hepática prévia
Grávidas ou mulheres em pós-parto
Com história de consumo de drogas
Com idade acima de 35 anos
A tomar outros fármacos hepatotóxicos ou com outras comorbilidades
O aparecimento de sintomas exige avaliação clínica e analítica.
]]>Comentário
O tratamento da tuberculose infecção latente é um progresso na abordagem da tuberculose, permitindo evitar casos de doença no futuro e, consequente, transmissão da doença.
O seu diagnóstico e tratamento devem, contudo, ser bem ponderados e orientados.
Bibliografia
1. American Academy of Pediatrics, Pediatric Tuberculosis Collaborative Group. Targeted tuberculin skin testing and treatment of latent tuberculosis infection in children and adolescents. Pediatrics 2004; 114: 1175-1201 (disponível em: http://www.pediatrics.org/cgi/content/full/114/4/S2/1175). [ Links ]
2. Sterling TR, Bethel J, Goldberg S, et al. The scope and impact of treatment of latent tuberculosis infection in the United States and Canada. Am J Respir Crit Care Med 2006; 173:927-931. [ Links ]
3. Ferebee SH. Controlled chemoprophylaxis trials in tuberculosis: a general review. Bibl Tuberc 1970; 26:28-106. [ Links ]
4. Hsu KH. Isoniazid in prevention and treatment of tuberculosis: a 20-year study of the effectiveness in children. JAMA 1974; 229:528-533. [ Links ]
5. International Union Against Tuberculosis. Efficacy of various durations of isoniazid preventive therapy for tuberculosis: five years of follow-up in the IUAT trial. Committee on Prophylaxis. Bull World Health Organ 1982; 60:555-564. [ Links ]
6. Mack U, Migliori GB, Sester M, Rieder HL, Ehlers S, Goletti D, Bossink A, Magdorf K, Hölscher C, Kampmann B, Arend SM, Detjen A, Bothamley G, Zellweger JP, Milburn H, Diel R, Ravn P, Cobelens F, Cardona PJ, Kan B, Solovic I, Duarte R, Cirillo DM; C. Lange; TBNET. LTBI: latent tuberculosis infection or lasting immune responses to M. tuberculosis? A TBNET consensus statement. Eur Respir J 2009; 33(5):956-973. [ Links ]
7. Starke JR. Current chemotherapy for tuberculosis in children. Infect Dis Clin North Am 1992; 6:215-235. [ Links ]
8. World Health Organizaiton. Treatment of tuberculosis: guidelines for national programmes. 3rd ed. Geneva: World Health Organization, 1997.
9. Ferebee SH. Controlled chemoprophylaxis trials in tuberculosis. A general review. Adv Tuberc Res 1969; 17:28-106. [ Links ]
10. Targeted tuberculin testing and treatment of latent tuberculosis infection. Am J Respir Crit Care Med 2000; 161:S221-S247. [ Links ]
11. Gutierrez EB, Gomes V, Picone CM, Suga H, Atomiya AN. Active tuberculosis and Mycobacterium tuberculosis latent infection in patients with HIV/ AIDS. HIV Med 2009; 10(9):564-572. [ Links ]
12. Lee SS, Chou KJ, Su IJ, Chen YS, Fang HC, Huang TS, Tsai HC, Wann SR, Lin HH, Liu YC. High prevalence of latent tuberculosis infection in patients in end-stage renal disease on hemodialysis: Comparison of QuantiFERON-TB GOLD, ELISPOT, and tuberculin skin test. Infection 2009; 37(2):96-102. [ Links ]
13. Jeon CY, Murray MB. Diabetes mellitus increases the risk of active tuberculosis: a systematic review of 13 observational studies. PLoS Med 2008; 5(7):e152. [ Links ]
14. Menzies D, Joshi R, Pai M. Risk of tuberculosis infection and disease associated with work in health care settings. Int J Tuberc Lung Dis 2007; 11(6):593-605. [ Links ]
15. Costa JT, Silva R, Sá R, Cardoso MJ, Ferreira J, Ribeiro C, Miranda M, Plácido JL. Tuberculosis Risk of continued transmission in healthcare workers. Ver Port Pneumol 2010; 16(1):5-21. [ Links ]
16. Hong Kong Chest Service/Tuberculosis Research Centre, Madras Medical Research Council, British Medical Research Council. A double-blind placebo-controlled clinical trial of three antituberculosis chemoprophylaxis regimens in patients with silicosis in Hong Kong. Am Rev Respir Dis 1992; 145:36-41. [ Links ]
17. Comstock G W, Baum C, Snider D E Jr. Isoniazid prophylaxis among Alaskan Eskimos: a final report of the Bethel Isoniazid Studies. Am Rev Respir Dis 1979; 119: 827-830. [ Links ]
18. Katz J, Kunofsky S, Damijonaitis V, Lafleur A, Caron T. Effect of isoniazid upon the reactivation of inactive tuberculosis. Final report. Am Rev Respir Dis 1965; 91:345-350. [ Links ]
19. Comstock G W, Ferebee S H, Hammes L M. A controlled trial of community-wide isoniazid prophylaxis in Alaska. Am Rev Respir Dis 1967; 95:935-943. [ Links ]
20. Spyridis NP, Spyridis PG, Gelesme A, Sypsa V, Valianatou M, Metsou F, Gourgiotis D, Tsolia MN. The effectiveness of a 9-month regimen of isoniazid alone versus 3 and 4-month regimens of isoniazid plus rifampin for treatment of latent tuberculosis infection in children: results of an 11-year randomized study. Clin Infect Dis 2007; 45(6):715 -722. [ Links ]
21. Menzies D, Long R, Trajman A, Dion MJ, Yang J, Al Jahdali H, Memish Z, Khan K, Gardam M, Hoeppner V, Benedetti A, Schwartzman K. Adverse events with 4 months of rifampin therapy or 9 months of isoniazid therapy for latent tuberculosis infection: a randomized trial. Ann Intern Med 2008;149(10):689-697. [ Links ]
22. Ijaz K, Jereb JA, Lambert LA, Bower WA, Spradling PR, McElroy PD, Iademarco MF, Navin TR, Castro KG. Severe or fatal liver injury in 50 patients in the United States taking rifampin and pyrazinamide for latent tuberculosis infection. Clin Infect Dis 2006; 42(3):346-355. [ Links ]
23. Centers for Disease Control and Prevention. Update: adverse event data and revised American Thoracic Society/CDC recommendations against the use of rifampin and pyrazinamide for treatment of latent tuberculosis infection in the United States, 2003. MMWR Morb Mortal Wkly Rep 2003; 52:735-739. [ Links ]
24. McElroy PD, Ijaz K, Lambert LA, et al. National survey to measure rates of liver injury, hospitalization, and death associated with rifampin and pyrazinamide for latent tuberculosis infection. Clin Infect Dis 2005; 41:1125-1133. [ Links ]
25. Gilroy SA, Rogers MA, Blair DC. Treatment of latent tuberculosis infection in patients aged > or =35 years. Clin Infect Dis 2000; 31(3):826-829. [ Links ]
26. Fountain FF, Tolley EA, Jacobs AR, Self TH. Rifampin hepatotoxicity associated with treatment of latent tuberculosis infection. Am J Med Sci 2009; 337(5):317-320. [ Links ]
27. Kopanoff DE, Snider DE Jr, Caras GJ. Isoniazid- related hepatitis: a U.S. Public Health Service cooperative surveillance study. Am Rev Respir Dis. 1978; 117(6):991-1001. [ Links ]
28. Snider DE Jr. Pyridoxine supplementation during isoniazid therapy. Tubercle 1980; 61(4):191-196. [ Links ]
29. Yew WW, Leung CC. Antituberculosis drugs and hepatotoxicity. Respirology 2006; 11(6):699-707. [ Links ]
30. Tostmann A, Boeree MJ, Aarnoutse RE, de Lange WC, van der Ven AJ, Dekhuijzen R. Antituberculosis drug-induced hepatotoxicity: concise up-to-date review. J Gastroenterol Hepatol 2008; 23(2):192-202. [ Links ]
Dra. Raquel Duarte
CDP Vila Nova de Gaia
]]> Rua Conselheiro VelosoVila Nova de Gaia
e-mail: raquelfduarte@gmail.com
Recebido para publicação: 25.01.10
Aceite para publicação: 11.05.10
]]>