Indicações para a abordagem cirúrgica da instabilidade anterior do ombro
Bernardo NunesI; Manuel GutierresI
I. Faculdade de Medicina da Universidade do Porto. Porto. Portugal.
RESUMO
]]> A Instabilidade Anterior do Ombro é uma lesão frequente e potencialmente incapacitante. Este trabalho visa compilar informação atualizada sobre a abordagem terapêutica desta patologia, visto que se trata de uma permanente fonte de controvérsia.Os avanços da artroscopia permitiram uma abordagem cirúrgica mini-invasiva, inicialmente apenas com o recurso à técnica de Bankart. Quando aplicada em pacientes com indicações precisas, apresenta taxas de recorrência relativamente baixas. Para a sistematização destas indicações, foi proposto o Instability and Severity Index Score (ISIS) que integra parâmetros como a idade, tipo de atividade desportiva, hiperlaxidex articular, assim como de lesões ósseas glenoidais ou umerais significativas. Um score <4 é habitualmente considerado como um valor limite para a utilização desta técnica, sendo no entanto possível, adicionar técnicas de plicatura ou capsulorrafia, com a finalidade de melhorar os resultados em casos selecionados.
Sendo assim, as técnicas de transferência da coracoide (como o Bristow-Latarjet), realizadas por via aberta ou artroscópica, continuam a ter um papel fundamental na maioria das situações onde a reconstrução anatómica não é suficiente para assegurar a prevenção desta recorrência.
Este trabalho realça a importância da seleção rigorosa da abordagem adequada a cada paciente de acordo com critérios clínicos e imagiológicos, em consonância com a diferenciação técnica do cirurgião. Mais do que uma opção entre cirurgia aberta vs artroscópica, a principal questão que se coloca é a decisão entre cirurgia de reconstrução anatómica das partes moles e as técnicas de batente ósseo. Não obstante, esta área carece de estudos mais homogéneos que permitam a comparação direta e a realização de meta-análises com maior acuidade.
Palavras chave: Luxação anterior do ombro, instabilidade anterior do ombro, reconstrução capsulolabral, Bankart, artroscopia, Bristow-Latarjet, indicações cirúrgicas.
ABSTRACT
Anterior Shoulder Instability is a frequent and potentially incapacitating injury. This paper aims to gather up to date information regarding the therapeutic approach of this pathology, as it is permanent matter of controversy.
Arthroscopy’s advances have allowed a mini-invasive surgical approach, initially only regarding Bankart technique. When used in patients with precise indications, it has revealed low recurrence rates. To allow for the systematization of these indications, the Instability and Severity Index Score was proposed, integrating criteria such as age, type of sports activity, shoulder hyperlaxity, as well as significant glenoid or umeral bony injuries. A score <4 is usually considered as the cut-off value for the use of this surgical technique. Nevertheless, it is also possible to add plicature or capsuloraphy techniques, in order to improve results in selected cases.
As such, coracoid transfer techniques (like Bristow-Latarjet), performed either via open surgery or arthroscopically, have remained to be fundamental in most situations where anatomical reconstruction is not enough to assure the prevention of recurrences.
]]> This paper highlights the importance of judicious selection of the appropriate approach to each patient, according to clinical and imaging criteria, and matching the surgeon’s technical differentiation. The main issue, more than an option between open or arthroscopic surgery, is deciding between anatomical reconstruction of soft tissue or bone-transfer techniques. Despite this, more homogeneous studies are lacking, to allow for direct comparisons and more accurate meta-analysis.Key words: Anterior dislocation of the shoulder, anterior instability of the shoulder, capsulolabral reconstruction, Bankart, Bristow-Latarjet, surgical indications.
INTRODUÇÃO
O ombro é a articulação mais móvel do corpo humano, sendo que este facto advém dum relativo sacrifício da estabilidade articular, tornando-a mais propensa a lesões que resultam em instabilidade articular[1,2], principalmente sob a forma de instabilidade anterior do ombro[3-5].
Após a recolha da história clínica e realização do exame físico, a caracterização imagiológica revela-se cada vez mais importante na definição da estratégia de reparação cirúrgica. Na maior parte dos casos, o recurso à radiografia simples complementa a avaliação da instabilidade para esclarecimento da direção da luxação e presença de lesões ósseas associadas[2,4]. Recomenda-se o uso de um conjunto de pelo menos 2 incidências (anteroposterior e lateral)[2], havendo no entanto alguns autores que sugerem um agrupado standard de 3 incidências (anteroposterior no plano escapular, axilar e apical oblíqua – incidência de Garth) [6]. A radiografia é frequentemente suficiente para o diagnóstico da lesão de Hill-Sachs, (descrita adiante). Neste caso, a incidência de Stryker é a que melhor avalia a presença, tamanho e orientação da lesão[7].
Outros meios auxiliares de diagnóstico podem caracterizar com maior precisão as lesões associadas, mas a sua utilização deve ser criteriosa. A Tomografia Computadorizada (TAC) destina-se a determinar a magnitude da perda óssea8, havendo autores que sugerem o recurso à TAC tridimensional com subtração digital da cabeça umeral[9-11]. Essa quantificação nomeadamente no que diz respeito à glenoide tem sido descrita de diversas formas: percentagem de Bankart ósseo em relação á área total de glenoide[12]; da área da sua porção inferior9; ou então simplesmente em relação ao diâmetro anteroposterior[13].
A Ressonância Magnética (RMN) é uma ferramenta útil para avaliar a integridade da coifa dos rotadores e estruturas ligamentares[9], como descrito mais à frente. Já o recurso a exames complementares com injeção de contraste – artroscanner ou artro-RMN – justificam-se em caso de necessidade de exploração adicional de determinadas variantes anatómicas ou laxidez capsular. No entanto, ainda que tanto a RMN como a artro-RMN sejam técnicas com grande precisão imagiológica no diagnóstico de lesões labrais e capsulares[14], a artroscopia continua a ser um importante complemento para uma correta decisão terapêutica[6].
LESÕES ARTICULARES ASSOCIADAS À INSTABILIDADE ANTERIOR
]]> A presença de lesões articulares associadas à instabilidade anterior do ombro é determinante na sua abordagem[2,4,15,16]. A lesão de Bankart - avulsão do labrum glenoidal, normalmente anteroinferior[4,17,18] - é a sequela mais comum[19]. Pode envolver apenas tecidos moles – Bankart “típico” – ou comprometer também uma fratura do bordo glenoidal anteroinferior, “arrancado” conjuntamente com a porção labral – Bankart ósseo – levando ao aspeto de “pera invertida” [8,20]. Apesar de ainda não haver um consenso na quantidade exata de perda óssea para uma lesão ser considerada significante, a maioria dos especialistas sugere entre 20% a 30% 8, com base nos resultados do desenvolvimento de instabilidade recidivante após a cirurgia de Bankart, reconstrutiva dos tecidos moles afetados. Ainda relacionada com as lesões de perda óssea glenoideia, Boileau et al descrevem um defeito ósseo por desgaste no rebordo glenoide anterior, que está associado a uma maior taxa de recidiva após a reconstrução de tecidos moles com a técnica de Bankart[21].Se ocorrer a avulsão da bainha periosteal do labrum anterior, ficamos perante uma variante da lesão de Bankart (lesão ALPSA), que condiciona um deslocamento inferomedial do labrum, com diminuição da restrição ao movimento de translação anterior da cabeça umeral e consequente luxação recidivante[16,20]. Esta última lesão pode ser eficazmente corrigida utilizando uma técnica artroscópica de mobilização de tecido do colo glenoidal, convertendo-a em lesão de Bankart “clássica”, com reparação e capsulorrafias subsequentes[16].
Por outro lado, a lesão de Bankart pode envolver estruturas mais superiores, acometendo a rutura do ligamento glenoumeral médio, o que resulta numa cicatrização mais frágil das estruturas, condicionando luxações recidivantes[4].
A lesão de Hill-Sachs[4,8,20] é a segunda lesão mais comum associada à instabilidade anterior do ombro [20], cuja extensão tem igualmente implicações prognósticas e na abordagem cirúrgica: lesões que afetem menos de 20% da curvatura da cabeça umeral não são normalmente causa significativa de instabilidade após técnica de reparação anatómica de tecidos moles[22, 23]; lesões com perda óssea superior a 40% estão diretamente relacionadas com instabilidade recidivante[21, 22]. A lesão de Hill-Sachs com 20% a 40% de perda óssea que cuja localização, orientação e “encaixe” da lesão no bordo glenoidal anteroinferior leve ao bloqueio da cabeça umeral na glenoide, conduz a instabilidade recidivante, e foi demonstrada uma alta taxa de falências após a reconstrução cirúrgica envolvendo apenas os tecidos moles anteriores[24].
Na avaliação da instabilidade anterior do ombro é também frequente encontrar algum grau de hiperlaxidez capsular, tanto anterior como posterior, resultante do movimento de translação excessivo que ocorre no evento inicial traumático, e sempre que as fibras constituintes não consigam retomar a tensão inicial[25,26].
A avulsão umeral dos ligamentos glenoumerais (HAGL) é outra lesão encontrada na instabilidade anterior e, caso presente, pode condicionar uma abordagem terapêutica especifica[27].
Para além do labrum inferior, também o labrum superior pode ser comprometido numa luxação anterior do ombro – a lesão SLAP (rutura do labrum superior anterior e posterior) [1]. O diagnóstico clínico desta lesão é ainda controverso. Apesar de haver alguma evidência que suporta que os testes de “Biceps Load I e II” [28], O´Brien e outros apresentam elevada especificidade e sensibilidade para esta lesão, outra revisão recente considera que apenas a combinação de vários destes testes permite a melhor acuidade deste diagnóstico[29].
TRATAMENTO CIRÚRGICO DA INSTABILIDADE ANTERIOR DO OMBRO
A abordagem cirúrgica da instabilidade anterior do ombro é feita, essencialmente, através de técnicas de reconstrução anatómica de tecidos moles, ou recorrendo a técnicas de batente ósseo.
]]> O procedimento de Bankart é um dos mais antigos na terapêutica desta patologia, consistindo na reconstituição anatómica do complexo capsulolabral[29,30]. A abordagem por cirurgia aberta com recurso a esta técnica foi considerada durante muitos anos o “gold-standard” para a correção cirúrgica da instabilidade glenoumeral, mas a sua adaptação para a via artroscópica e posterior desenvolvimento levaram à disseminação do uso da artroscopia nesta patologia[31,32]. Este procedimento permite também diminuir a laxidez capsular excessiva causada pela instabilidade recidivante adicionando uma capsulorrafia descrita por Neer[33]. A plicatura capsular posterior pode ser associada ao procedimento de Bankart, de forma a diminuir a laxidez do complexo capsulo-labral inferior, uma vez que também o feixe posterior do ligamento gleoumeral inferior é lesado no evento que leva à instabilidade anterior, com resultante redundância capsular[34]. Tenta-se assim obter um correto balanço ligamentar das estruturas não só anteriores como da região posterior.As técnicas de Latarjet e Bristow, dantes tipicamente usadas por via aberta através duma incisão deltopeitoral, assemelham-se na medida em que ambas recorrem à osteotomia e transferência da ponta da apófise coracoide e tendões nela inseridos, para a superfície anterior do colo glenoidal, através do recurso a parafusos. A diferença entre ambas situa-se na posição do enxerto coracoide, uma vez que a técnica de Bristow posiciona o maior eixo do enxerto perpendicularmente[35], enquanto a de Latarjet o posiciona paralelamente à glenoide[36]. Atualmente é já possível efetuar artroscopicamente estas técnicas de enxerto ósseo[36, 37]. No entanto, mantém ainda elevada dificuldade técnica, mesmo com recurso a instrumentais especificos, e carecem de resultados a médio e longo prazo. Não obstante, é aguardado com expectativa o desenvolvimento da experiência e adequação do hardware, existindo possibilidades para a generalização do seu uso num futuro próximo[36].
Em casos de lesões de Hill-Sachs com perda óssea significativa e consequente “encaixe”, foi recentemente desenvolvida uma técnica denominada de “remplissage” [6], que consiste no preenchimento do defeito da cabeça umeral por cápsula posterior e “tenodesis” do infraespinhoso, por via artroscópica[38].
O procedimento de Putti-Platt e a técnica de Magnuson-Stack estiveram associadas a taxas de complicações e recidiva elevadas que conduziram ao seu abandono[39-43].
Até ao momento, continua a existir muita controvérsia em relação a qual o melhor procedimento para a abordagem cirúrgica da instabilidade anterior do ombro – reconstrução anatómica ou uso de batente ósseo – assim como o momento em que este deve ser considerado.
Em relação ao momento da cirurgia, alguns autores recomendam a intervenção precoce em pacientes jovens e ativos (após o 1º episódio de luxação), devido à elevada taxa de reincidências neste grupo, ao maior desgaste das estruturas ligamentares, e à eventual presença de lesões de Hill-Sachs com o decorrer do tempo[4,44,45]. No entanto, dois argumentos contra esta abordagem parecem ganhar maior consenso entre os clínicos. O primeiro consiste na interpretação das taxas de recidiva, sem tratamento cirúrgico, após o evento inicial: cerca de 50-60%. Isto significa que seriam operados metade dos pacientes sem que estes fossem desenvolver instabilidade recidivante no futuro, aumentando o risco iatrogénico[46]. O segundo argumento prende-se com a possibilidade de ocorrência de complicações cirúrgicas tardias, como a perda de amplitude de movimentos, que condicionam e exigem ponderação na decisão de avançar com a cirurgia[2].
RECONSTRUÇÃO ANATÓMICA vs BATENTE ÓSSEO
A cirurgia de Bankart, atualmente realizada quase exclusivamente por artroscopia, reúne as vantagens desta abordagem, como a sua natureza relativamente atraumática que dispensa a incisão do subscapular,; tempo de internamento e recuperação mais curtos, com retorno mais rápido ao trabalho e à atividade física; incisões menores com melhor resultado cosmético; menor dor; e melhor recuperação da amplitude de movimento e função[2,32,47,48].
As desvantagens apontadas a este procedimento são taxas de recidiva possivelmente superiores às das cirurgias de batente ósseo[2], justificadas por uma curva de aprendizagem morosa e indicações erradas, como sejam a incapacidade de reconhecer a presença de lesões ósseas significativas[48]. Estudos recentes mostram taxas de recidiva significativamente baixas, após aplicarem critérios de seleção para incluir os pacientes numa intervenção artroscópica de reparação anatómica[15]. Thomazeau et al obtiveram um resultado de 3.2% de recidivas, ao fim de 18 meses[15]. Porcellini, com um follow-up médio de 3 anos, não encontrou nenhum caso de recidiva, após ter utilizado a artroscopia apenas em pacientes com Bankart ósseo inferior a 25%[49], o que reforça as conclusões de Mologne et al e Burkhartt et al. No primeiro, a taxa de recidiva de 14,3% encontrada após artroscopia pôde ser reduzida a 0% caso se considerassem apenas os casos em que o fragmento ósseo foi incorporado na reparação[50]. No segundo, a taxa de recidiva após artroscopia variou entre 67%, em pacientes com perda óssea significativa, e 4%, em pacientes com diminuta lesão óssea glenoidal[24]. A meta-análise recente de Petrera é cabal neste aspeto: a taxa de recidiva diminui de um total de 4.7% - considerando todos os estudos analisados- para 2.9% na artroscopia se atentarmos apenas aos estudos com data posterior a 2002 (que incluem já algumas indicações para cada procedimento) [48].
]]> Em relação aos índices de satisfação do paciente, averiguados por diferentes escalas (Rowe, Walch-Duplay, escala de dor VAS), a análise da literatura permite concluir que o Bankart artroscópico apresenta scores equivalentes ou superiores às técnicas de cirurgia aberta (de Bankart ou batente ósseo) [15,32,51]. Ressalva-se, no entanto, que as diferentes escalas utilizadas nos vários artigos dificultam a comparação do grau de satisfação dos pacientes após a cirurgia[48]. Complementarmente, o estudo de Porcellini demonstrou um regresso de 92% dos pacientes ao mesmo nível de competição prévio à intervenção artroscópica, em atletas com Bankart ósseo inferior a 25%[49].A cirurgia de batente ósseo tem como vantagens uma taxa de recidivas reconhecidamente baixa[4], mas apresenta-se com uma maior taxa de complicações pós-operatórias, nas quais se inclui alguma perda de amplitude de movimentos[6,20,48], maior tempo de internamento e recuperação[20], e incidência superior de artrose glenoumeral[6]. Isto foi descrito para procedimentos realizados pela via aberta convencional, aguardando-se com expectativa os resultados a longo prazo dos estudos efetuados em pacientes sujeitos a esta intervenção por artroscopia[36, 37].
As técnicas não-anatómicas de correção de instabilidade (Bristow-Latarjet) apresentam baixas taxas de recidiva, mesmo em estudos com longos períodos de seguimento. Young et al demonstraram menos de 1% de recidivas em mais de 2000 procedimentos[52], e o estudo randomizado de Fabricciani não encontrou recidivas após 2 anos[53]. Com maior período de seguimento, destacam-se os valores de 13,6% aos 15 anos, com apenas um caso que necessitou de cirurgia de revisão[54], 5% após 6 anos, em pacientes com perda óssea glenoidal significativa[55], e de 0% após uma média de 14,3 anos de follow-up, em que 96% dos ombros tinham lesão óssea significativa[56].
As escalas de subjetividade analisadas demonstram resultados semelhantes ou inferiores à cirurgia artroscópica, com resultados bons ou excelentes de 70-98%, dependendo também da escala utilizada[52,53,56,57].
Em relação às complicações, verificou-se uma alta incidência de artrose (40-60%) em alguns estudos que avaliaram os resultados das técnicas de Bristow-Latarjet[54, 56, 67,69], mas outros mais recentes demonstraram uma incidência desta semelhante à da reconstrução anatómica por via aberta[65]. Ambas as técnicas estão associadas à perda de algum grau de amplitude de movimentos do ombro, principalmente da rotação externa (entre 5-11º) [68,69,71].
O regresso ao mesmo nível competitivo prévio à cirurgia foi verificado em 83% dos casos, segundo a revisão de Young et al[52].
Por estas razões torna-se importante definir com maior exatidão os critérios e situações nas quais a reconstrução anatómica pode ser maximizada, e aquelas onde esta é insuficiente para assegurar a estabilidade articular, devido à presença de outras lesões associadas.
INDICAÇÕES PARA REPARAÇÃO DA INSTABILIDADE ANTERIOR DO OMBRO
A intervenção cirúrgica deve ser recomendada, em geral, a pacientes com instabilidade recidivante, dor, ou limitações da atividade (desportiva ou ocupacional), após um período de tratamento conservador que se revelou incapaz de debelar estas condicionantes[2].
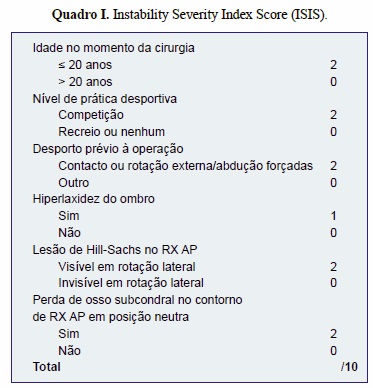
]]> Com o objetivo de apresentar indicações específicas para a escolha da técnica de Bankart artroscópica, foram estabelecidos os critérios ISIS (Instability Severity Index Score) [58], que se revelaram fiáveis nos seus resultados iniciais, uma vez que a sua aplicação revelou uma baixa recidiva (3,2%) nos pacientes selecionados para a reparação de Bankart artroscópica, assim como elevados valores de satisfação subjetiva do paciente, como avaliado pelas escalas de Rowe e Walch-Duplay[15].Os critérios ISIS consistem num sistema de pontuação com um valor máximo de 10 pontos, conferidos pela presença de determinados fatores. Os dados da história e exame físico consistem em: idade na altura da cirurgia, nível de atividade física, tipo de desporto praticado antes da cirurgia e hiperlaxidez do ombro (definida pela rotação externa superior a 85º com o cotovelo encostado ao corpo e/ ou teste de hiperabdução maior que 90º). Os achados imagiológicos relevantes são a presença de lesão de Hill-Sachs no RX e perda do contorno ósseo subcondral (Quadro I) [58]. Inicialmente, a atribuição de um score superior a 6 valores recomendava a opção por uma técnica de reconstrução não-anatómica, nomeadamente a transferência de coracoide de Bristow-Latarjet, uma vez que, nestes casos, a simples reconstrução dos tecidos moles parece insuficiente para assegurar a estabilidade articular sem recidivas. Esta indicação foi posteriormente adaptada e o estudo de Thomazeau et al, publicado em 2010 demonstrou excelentes resultados ao atribuir a via artroscópica a pacientes com ISIS ≤ 4 e a técnica de Bristow-Latarjet nos restantes[15].
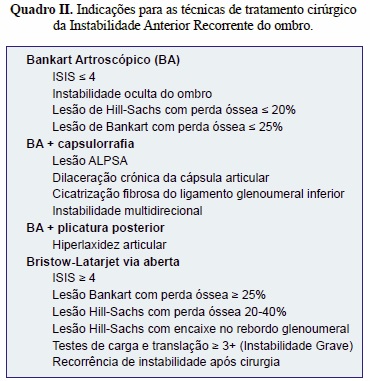
No entanto, fazendo uma análise atenta da literatura, parece ser possível identificar algum consenso entre os artigos de revisão, permitindo reunir indicações complementares àquelas dos critérios ISIS, e que estão resumidas no Quadro II. Assim, a reconstrução de Bankart artroscópica deve ser utilizada em pacientes que apresentem instabilidade oculta do ombro (vide-supra) [4], lesões de Hill-Sachs com perda óssea quantificada como inferior a 20%[21,24,59-61] e lesões de Bankart ósseas com perda óssea inferior a 25% da largura glenoidal, sendo que neste caso, é necessária a reintegração do fragmento ósseo original. Caso contrário a reconstrução não-anatómica é a mais recomendada[6].
Existem outras situações onde a reconstrução de Bankart necessita ser complementada com uma capsulorrafia de Neer (“Neer capsular shift”). Nestas incluem-se:
1) as lesões ALPSA (suprarreferidas), com mobilização do tecido do colo glenoidal, convertendo a lesão num “Bankart típico”, e posterior reconstrução e capsulorrafia[16].
2) a dilaceração crónica da cápsula ou a cicatrização fibrosa do ligamento glenoumeral inferior[4];
3) instabilidade multidirecional[2].
Como já referido neste artigo, a resolução do problema da distensão posterior da cápsula aquando da sua luxação anterior passa pela utilização da técnica de plicatura posterior, como complemento à técnica de Bankart, por via artroscópica. Estudos efetuados mostram uma melhoria dos scores subjetivos – ASES – mas carecem ainda de mais evidência que o comprovem de forma categórica[34].
Não obstante um alargado leque de recomendações que aconselham quais os pacientes a incluir numa reparação anatómica, as técnicas de “batente ósseo” – Bristow e Latarjet – são também bastante relevantes.
O ISIS aponta o recurso a estas técnicas caso se verifique um score superior a 4[15]. Complementarmente, as revisões efetuadas neste âmbito quantificam as perdas ósseas que justifiquem esta intervenção e acrescentam algumas indicações:
1) perda óssea glenoidal superior a 25% (aspeto da “pera invertida) [8];
2) lesões de Hill-Sachs com perda óssea entre 20- 40% ou “engaging” [8, 52];
3) lesões ósseas glenoidais e umerais conjuntas[52]; 4) recidiva da instabilidade, mesmo após cirurgia artroscópica[20].
Relativamente às lesões de Hill-Sachs, a literatura mais recente aconselha que nas situações em que se verifique uma perda óssea de 20-40% se complemente a técnica de Bristow-Latarjet com uma “remplissage” efetuada artroscopicamente, ou através do preenchimento da lesão com auto ou aloenxertos[8,10,38,62,63]. As perdas ósseas superiores a 40%, são de difícil solução, podendo ser ponderada a realização de uma hemi-artroplastia[6,8].
CONCLUSÃO
A Instabilidade Anterior Recorrente do Ombro é um problema comum e alvo de grande investigação. De facto, a sua abordagem cirúrgica é um tema vasto e controverso, existindo um sem número de estudos sobre o assunto. No entanto, da análise objetiva destas publicações resulta que a maior parte destas se tratam de estudos retrospetivos com muitas falhas metodológicas, que tornam difícil a sua comparação e extrapolação de resultados.
Desta forma, a pesquisa bibliográfica teve de ser efetuada criteriosamente, atentando aos métodos utilizados e analisando criticamente as conclusões apresentadas.
A mais-valia desta revisão é a compilação num só artigo de informação recente no que concerne às indicações para a abordagem cirúrgica da instabilidade anterior do ombro. De facto, existem já evidências que recomendam a cirurgia de Bankart artroscópica para determinados subgrupos de doentes, com resultados iguais ou superiores à cirurgia com recurso a batente ósseo, aos quais se juntam as vantagens da abordagem mini-invasiva da artroscopia. Para além disso, neste artigo também se concluíram quais as lesões que devem ser encaminhadas diretamente para uma intervenção de reconstrução não-anatómica - Bristow-Latarjet - esclarecendo assim o papel de ambas as abordagens para a obtenção dos melhores resultados, suportados pelas evidências científicas. Percebe-se assim a importância da correta avaliação préoperatória na definição do tipo de abordagem a efetuar. Com o aprimoramento dos sistemas de classificação como o ISIS, poderemos assistir a uma melhoria ainda maior dos resultados dos procedimentos artroscópicos, como se depreende dos estudos efetuados para definir estes valores de “cut-off”, e assim potenciar as vantagens da cirurgia artroscópica com um menor número de recidivas – escolher o procedimento certo, para o paciente certo. Desta forma, assistimos a uma mudança do paradigma de controvérsia de cirurgia aberta ou artroscópica, para uma dicotomia entre reconstrução anatómica ou de batente ósseo, com o eventual recurso, em ambas, à abordagem artroscópica.
Em suma, é atualmente possível identificar critérios clínicos e imagiológicos objetivos que permitam selecionar uma abordagem cirúrgica para cada situação de instabilidade anterior recorrente do ombro, no sentido de maximizar os resultados e satisfação dos pacientes.
]]> Importa salientar que é ainda necessária uma maior uniformização no desenho dos estudos neste campo, para que da sua comparação seja possível extrair níveis máximos de evidência.
REFERÊNCIAS BIBLIOGRÁFICAS
1. Prescher A. Anatomical basics, variations, and degenerative changes of the shoulder joint and shoulder girdle. European journal of radiology. 2000; 35: 88-102 [ Links ]
2. Wen D. Y.. Current concepts in the treatment of anterior shoulder dislocations. The American journal of emergency medicine. 1999; 17: 401-407 [ Links ]
3. Chalidis B.. Has the management of shoulder dislocation changed over time?. International orthopaedics. 2007; 31: 385-389 [ Links ]
4. Blum A., Coudane H., Molé D.. Gleno-humeral instabilities. European radiology. 2000; 10: 63-82 [ Links ]
5. Rowe C. R.. Acute and recurrent anterior dislocations of the shoulder. The Orthopedic clinics of North America. 1980; 11: 253-270 [ Links ]
6. Lynch J. R., Clinton J. M., Dewing C. B., Warme W. J., Matsen F. A.. Treatment of osseous defects associated with anterior shoulder instability. Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons. 18: 317-328 [ Links ]
7. HALL R. H., ISAAC F., BOOTH C. R.. Dislocations of the shoulder with special reference to accompanying small fractures. The Journal of bone and joint surgery American. 1959; 41-A: 489-494 [ Links ]
8. Bollier M. J., Arciero R.. Management of glenoid and humeral bone loss. Sports medicine and arthroscopy review. 2010; 18: 140-148 [ Links ]
9. Piasecki D. P.. Glenoid bone deficiency in recurrent anterior shoulder instability: diagnosis and management. The Journal of the American Academy of Orthopaedic Surgeons. 2009; 17: 482-493 [ Links ]
10. Bushnell B. D., Creighton R. A., Herring M. M.. Bony instability of the shoulder. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2008; 24: 1061-1073 [ Links ]
11. Chuang T.-Y., Adams C. R., Burkhart S. S.. Use of preoperative three-dimensional computed tomography to quantify glenoid bone loss in shoulder instability. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2008; 24: 376-382 [ Links ]
12. Provencher M. T.. Recurrent shoulder instability: current concepts for evaluation and management of glenoid bone loss. The Journal of bone and joint surgery American. 2010; 92 (2): 133-51 [ Links ]
13. Gerber C., Nyffeler R. W.. Classification of glenohumeral joint instability. Clinical orthopaedics and related research. 2002; : 65-76 [ Links ]
14. Steinbach L. S.. MRI of shoulder instability. European journal of radiology. 2008; 68: 57-71 [ Links ]
15. Thomazeau H.. Can we improve the indication for Bankart arthroscopic repair? A preliminary clinical study using the ISIS score. Orthopaedics & traumatology, surgery & research : OTSR. 2010; 96: 77-83 [ Links ]
16. Neviaser T. J.. The anterior labroligamentous periosteal sleeve avulsion lesion: a cause of anterior instability of the shoulder. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 1993; 9: 17-21 [ Links ]
17. Rowe C. R., Patel D., Southmayd W. W.. The Bankart procedure: a long-term end-result study. The Journal of bone and joint surgery American. 1978; 60: 1-16 [ Links ]
18. Urayama M., Itoi E., Sashi R., Minagawa H., Sato K.. Capsular elongation in shoulders with recurrent anterior dislocation. Quantitative assessment with magnetic resonance arthrography. The American journal of sports medicine. 31: 64-67 [ Links ]
19. Rockwood Charles A, Jr., Matsen Frederick A, III, Wirth Michael A., Lippit Steven B., Fehringer Edward V., Sperling J. W.. Rockwood: The Shoulder. Philadelphia: Saunders Elsevier; 2009. [ Links ]
20. Pope E. J., Ward J. P., Rokito A. S.. Anterior shoulder instability - a history of arthroscopic treatment. Bulletin of the NYU hospital for joint diseases. 2011; 69: 44-49 [ Links ]
21. Boileau P.. Risk factors for recurrence of shoulder instability after arthroscopic Bankart repair. The Journal of bone and joint surgery. American volume. 2006; 88: 1755-1763 [ Links ]
22. Chen A. L., Hunt S. A., Hawkins R. J., Zuckerman J. D.. Management of bone loss associated with recurrent anterior glenohumeral instability. The American journal of sports medicine. 2005; 33: 912-925 [ Links ]
23. Taylor D. C., Arciero R. A.. Pathologic changes associated with shoulder dislocations. Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. The American journal of sports medicine. 25: 306-311 [ Links ]
24. Burkhart S. S., De Beer J. F.. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2000; 16: 677-694
25. Bigliani L. U.. Tensile properties of the inferior glenohumeral ligament. Journal of orthopaedic research : official publication of the Orthopaedic Research Society. 1992; 10: 187-197 [ Links ]
26. Speer K. P.. Biomechanical evaluation of a simulated Bankart lesion. The Journal of bone and joint surgery. American volume. 1994; 76: 1819-1826 [ Links ]
27. Matsen F. A., Chebli C., Lippitt S.. Principles for the evaluation and management of shoulder instability. The Journal of bone and joint surgery. American volume. 2006; 88: 648-659 [ Links ]
28. Munro W., Healy R.. The validity and accuracy of clinical tests used to detect labral pathology of the shoulder - a systematic review. Manual therapy. 2009; 14: 119-130 [ Links ]
29. Bankart A. S.. RECURRENTOR HABITUAL DISLOCATION OF THE SHOULDER-JOINT. British medical journal. 1923; 2: 1132-1133 [ Links ]
30. Bankart A. S. B.. The pathology and treatment of recurrent dislocation of the shoulder-joint. British Journal of Surgery. 1938; 26: 23-29 [ Links ]
31. Cole B. J., Insalata J. L., Irrgang J., Warner J. J. P.. Comparison of Arthroscopic and Open Anterior Shoulder Stabilization : A Two to Six-Year Follow-up Study Comparison of Arthroscopic and Open Anterior Shoulder Stabilization. 2011; [ Links ]
32. Mahiroğulları M.. Comparison between the results of open and arthroscopic repair of isolated traumatic anterior instability of the shoulder. Acta orthopaedica et traumatologica turcica. 2010; 44: 180-185 [ Links ]
33. Neer C. S., Foster C. R.. Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder. A preliminary report. The Journal of bone and joint surgery. American volume. 1980; 62: 897-908 [ Links ]
34. Westerheide K. J., Dopirak R. M., Snyder S. J.. Arthroscopic anterior stabilization and posterior capsular plication for anterior glenohumeral instability: a report of 71 cases. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2006; 22: 539-547 [ Links ]
35. HELFET A. J.. Coracoid transplantation for recurring dislocation of the shoulder. The Journal of bone and joint surgery. British volume. 1958; 40-B: 198-202 [ Links ]
36. Lafosse L., Boyle S.. Arthroscopic Latarjet procedure. Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons. 2010; 19: 2-12 [ Links ]
37. Taverna E., Golanò P., Pascale V., Battistella F.. An arthroscopic bone graft procedure for treating anterior-inferior glenohumeral instability. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2008; 16: 872-875 [ Links ]
38. Purchase R. J., Wolf E. M., Hobgood E. R., Pollock M. E., Smalley C. C.. Hill-sachs "remplissage": an arthroscopic solution for the engaging hill-sachs lesion. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2008; 24: 723-726 [ Links ]
39. Leach R. E., Corbett M., Schepsis A., Stockel J.. Results of a modified Putti-Platt operation for recurrent shoulder dislocations and subluxations. Clinical orthopaedics and related research. 1982; : 20-5 [ Links ]
40. Collins K. A., Capito C., Cross M.. The use of the Putti-Platt procedure in the treatment of recurrent anterior dislocation. With special reference to the young athlete. The American journal of sports medicine. 14: 380-382 [ Links ]
41. Fredriksson A. S., Tegner Y.. Results of the Putti-Platt operation for recurrent anterior dislocation of the shoulder. International orthopaedics. 1991; 15: 185-188 [ Links ]
42. Hawkins R. J., Angelo R. L.. Glenohumeral osteoarthrosis. A late complication of the Putti-Platt repair. The Journal of bone and joint surgery. American volume. 1990; 72: 1193-1197 [ Links ]
43. Hale J., Rokito A. S., Chu J.. Anterior capsulolabral reconstruction for traumatic recurrent anterior shoulder dislocation. Bulletin (Hospital for Joint Diseases (New York, N.Y.)). 2005; 62: 94-98 [ Links ]
44. Spatschil A. Posttraumatic anterior-inferior instability of the shoulder: arthroscopic findings and clinical correlations. Archives of orthopaedic and trauma surgery. 2006; 126: 217-222 [ Links ]
45. Boone J. L., Arciero R. A.. First-time anterior shoulder dislocations: has the standard changed?. British journal of sports medicine. 2010; 44: 355-360 [ Links ]
46. Kuhn J. E.. Treating the initial anterior shoulder dislocation- -an evidence-based medicine approach. Treating the initial anterior shoulder dislocation - an evidence-based medicine approach. 2006; 14: 192-198
47. Cole B. J., L'Insalata J., Warner J. J.. Comparison of arthroscopic and open anterior shoulder stabilization. A two to six-year follow-up study. The Journal of bone and joint surgery. American volume. 2000; 82-A: 1108-1114 [ Links ]
48. Petrera M., Patella V., Patella S., Theodoropoulos J.. A meta-analysis of open versus arthroscopic Bankart repair using suture anchors. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2010; 18: 1742-1747 [ Links ]
49. Porcellini G., Campi F., Paladini P.. Arthroscopic approach to acute bony Bankart lesion. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2002; 18: 764-769 [ Links ]
50. Mologne T. S., Provencher M. T., Menzel K. A., Vachon T. A., Dewing C. B.. Arthroscopic stabilization in patients with an inverted pear glenoid: results in patients with bone loss of the anterior glenoid. The American journal of sports medicine. 2007; 35: 1276-1283 [ Links ]
51. Lenters T. R., Franta A. K., Wolf F. M., Leopold S. S., Matsen F. A.. Arthroscopic compared with open repairs for recurrent anterior shoulder instability. A systematic review and meta-analysis of the literature. The Journal of bone and joint surgery. American volume. 2007; 89: 244-254 [ Links ]
52. Young A. A., Maia R., Berhouet J., Walch G.. Open Latarjet procedure for management of bone loss in anterior instability of the glenohumeral joint. Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons. 2011; 20: 61-69 [ Links ]
53. Fabbriciani C.. Arthroscopic versus open treatment of Bankart lesion of the shoulder: a prospective randomized study. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2004; 20: 456-462 [ Links ]
54. Hovelius L.. Recurrences after initial dislocation of the shoulder. Results of a prospective study of treatment. The Journal of bone and joint surgery. American volume. 1983; 65: 343-349 [ Links ]
55. Burkhart S. S.. Results of modified Latarjet reconstruction in patients with anteroinferior instability and significant bone loss. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2007; 23: 1033-1041 [ Links ]
56. Allain J., Goutallier D., Glorion C.. Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder. The Journal of bone and joint surgery. American volume. 1998; 80: 841-852 [ Links ]
57. Schroder D. T., Provencher M. T., Mologne T. S., Muldoon M. P., Cox J. S.. The modified Bristow procedure for anterior shoulder instability: 26-year outcomes in Naval Academy midshipmen. The American journal of sports medicine. 2006; 34: 778-786 [ Links ]
58. Balg F., Boileau P.. The instability severity index score. A simple pre-operative score to select patients for arthroscopic or open shoulder stabilisation. The Journal of bone and joint surgery. British volume. 2007; 89: 1470-1477 [ Links ]
59. Itoi E.. A new method of immobilization after traumatic anterior dislocation of the shoulder: a preliminary study. Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons. 12: 413-415 [ Links ]
60. Yamamoto N.. Effect of an anterior glenoid defect on anterior shoulder stability: a cadaveric study. The American journal of sports medicine. 2009; 37: 949-954 [ Links ]
61. Abrams J. S.. Role of arthroscopy in treating anterior instability of the athlete's shoulder. Sports medicine and arthroscopy review. 2007; 15: 230-238 [ Links ]
62. Ochoa E., Burkhart S. S.. Glenohumeral bone defects in the treatment of anterior shoulder instability. Instructional course lectures. 2009; 58: 323-336 [ Links ]
63. Toro F.. Remplissage: Infraspinatus Tenodesis and Posterior Capsulodesis for the Treatment of Hill Sachs Lesions. Techniques in Shoulder and Elbow Surgery. 2008; 9: 188-192 [ Links ]
Conflito de interesse:
]]> Nada a declarar.
Bernardo Nunes
Faculdade de Medicina da Universidade
do Porto
Alameda Prof. Hernâni Monteiro
4200 - 319 Porto
Portugal
jbernardo.m.nunes@gmail.com
Data de Submissão: 2013-02-01
Data de Revisão: 2013-08-09
Data de Aceitação: 2013-08-19
]]>