Acute fatty liver of pregnancy - case report
Esteatose hepática aguda da gravidez - caso clínico
Fernanda Vilela*, Ana Edral*, Rita Martins*, Amália Pacheco**
Serviço de Obstetrícia do Centro Hospitalar do Algarve - Unidade de Faro
*Interna de formação específica de Ginecologia e Obstetrícia
**Assistente Hospitalar Graduada de Ginecologia e Obstetrícia
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
]]> Acute fatty liver of pregnancy (AFLP) is a rare and life-threatening disorder. The etiology of AFLP is still unclear, however recent studies demonstrated association with long-chain 3-hydroxyacyl-CoA dehydrogenase deficiency1-3.In this report we describe a 27-year-old woman that presented at 38 weeks of gestation in spontaneous labour. She underwent emergency caesarean for non-reassuring fetal heart tracing. After caesarean the patient developed confusion, tremor, vomits and pruritus. She also presented jaundice and choluria. Laboratory data revealed hepatic dysfunction and imaging exams demonstrated hepatic lipid infiltration. The diagnosis of AFLP was defined based on clinical, laboratory and ultrasound findings and was confirmed by liver biopsy. She was successfully treated with supportive therapy.
This case report reinforces the importance of recognition of clinical, laboratory and imaging findings suggestive of AFLP and demonstrates that early diagnosis and prompt supportive therapy improve the outcome reducing maternal and neonatal mortality1,4.
Keywords: Fatty liver; Pregnancy.
Introduction
Acute fatty liver of pregnancy (AFLP) is a rare and life-threatening disorder that affects 1 in 13000 pregnancies1,2. It was first described as acute yellow atrophy of the liver in pregnancy in 1940 by Sheehan2.
AFLP usually occurs at third trimester (between 30 and 38 weeks of gestation) or during postpartum period1-3. This clinical condition may return at subsequent pregnancies and is more common in underweight women, primigravidas, male fetus and multiple gestations2,4,5. There aren't any geographical or ethnicity differences in AFLP3.
The etiology and pathogenesis of AFLP remains unknown but recent studies suggested that dysfunction of beta-oxidation of long chain fatty acids could be involved2,4. Long-chain 3-hydroxyacyl-CoA dehydrogenase (LCHAD) is a mitochondrial enzyme involved in fatty acid oxidation that is the primary mechanism of ketone bodies production. Ketone bodies are the major source of energy for the brain and heart when glucose blood levels are low, for example during prolonged fasting2.
Fetuses with LCHAD deficiency have impaired fatty acid oxidation and produce toxic metabolites that accumulate in maternal circulation and liver causing toxicity. In a heterozygous mother for LCHAD mutation, the capacity to metabolize long chain fatty acids is reduced because of impaired enzyme function. The metabolic stress of pregnancy (specially at third trimester) in a susceptible mother carrying a LCHAD deficient fetus leads to progressive microvesicular fatty infiltration at hepatocytes2,5,6.
]]> Clinical and laboratory findings in AFLP are non-specific which difficult the differential diagnosis from other pregnancy disorders such as pre-eclampsia, viral hepatitis, hepatotoxicity or cholestasis4,6-8. The most common presentation is jaundice, nausea, vomiting, confusion, headache and fatigue. Abdominal pain appears particularly at the epigastric area and right upper quadrant1,4,6,8. Disseminated intravascular coagulation (DIC) is a common complication affecting 75-80% of the patients3,6. Coagulopathy in AFLP results from deficient production of pro-coagulant factors and increased use by intravascular coagulation12. Other systemic complications in AFLP include encephalopathy, acute renal failure, infection, pancreatitis, gastrointestinal hemorrhage and respiratory or hepatic failure8,10,11.Laboratory findings usually include elevated aminotransferases (300 U/L to 500 U/L but can reach 1.000 U/L), elevated bilirubin, ammonia, uric acid and alkaline fosfatase (10 times normal). Other findings like abnormal prothrombine time, leukocytosis, and thrombocytopenia can be present1,4,7,8. Because of impaired glicogenolysis, hypoglycaemia can also occur in severe cases of hepatic function impairment1,3.
The diagnosis of AFLP can be established based on clinical, laboratory and imaging findings. Liver biopsy is the goldstandart diagnostic test but is not recommended at more severe cases due to the high risk of bleeding3,4,7.
AFLP has high maternal and perinatal morbidity and mortality. However, early detection and appropriate management has improved the prognosis. Treatment of acute fatty liver during pregnancy consists in prompt delivery and maternal supportive care4,7,8. After an AFLP episode is important to test the mother and the newborn for LCHAD mutations to genetic counselling in subsequent pregnancies2,7,8.
Case Report
A 27-year-old, caucasian woman, gravida 2 para 1, was admitted at obstetric emergency with 38 weeks of gestation at beginning of labour. On admission normal blood pressure was observed and the laboratory results demonstrated normal hematologic findings with a slightly increase of protrombine time.
Prior medical history and family history were unremarkable. The previous pregnancy and labour occurred without complications.
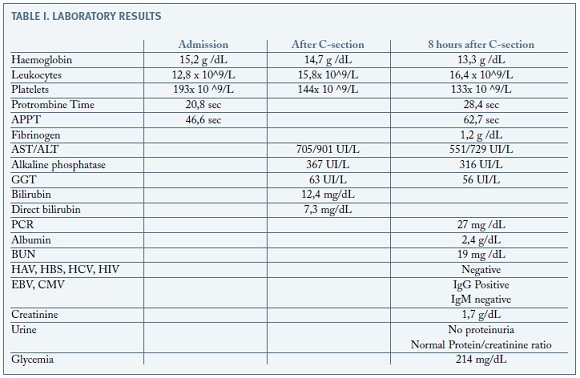
During the beginning of active fase of labour, continuous cardiotocography monitoring showed repetitive late decelerations with reduced variability (CTG type III). Due to non-reassuring fetal heart tracing the patient underwent emergency caesarean section. The procedure went without complications. The outcome was a feminine newborn with 3480g and Apgar score of 3 at 1st minute, 7 at 5ft minute and 9 at 10th minute. She was reanimated after birth and went to the neonatal intensive care unit (NICU). During caesarean it was noticed maternal jaundice and choluria. Posto perative blood tests demonstrated elevated aminotransferases (AST 705 UI/L ( N 5-34); ALT 901 UI/L (N<55)), alkaline fosfatase (367 U/L ( N 40-150)) and bilirubin ( 12,4 mg/dL (N 0,20-1,20 mg/dL) (Table I).
]]>
8 hours after c-section the patient presented confusion, slurred speech and tremor. She also referred vomits and dizziness. She denied have taken any medication, drugs or teas during pregnancy. At physical examination we found impaired awareness, jaundice, tachycardia and tremor without flapping. The laboratory findings were as follows: Hb 13,3 g/dL, platelets 133 x 109/L, PT 28.4sec, APTT 62,7sec, albumin 2,4 g/dL, AST 551 IU/L, ALT 729 IU/L, creatinine 1,70 mg/dL. Serum fibrinogen was reduced. HVA, HVB, HVC, CMV, EBV and HIV 1/2 laboratory screening was negative. The patient present normal blood pressure and no proteinuria or increased ratio proteins/ /creatinine (Table I).
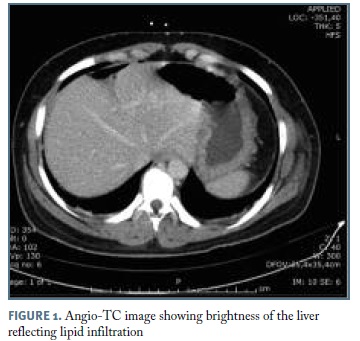
Abdominal ultrasound revealed mild hepatic steatosis without suggestive findings of cholestasis or thrombosis. Hepatic heterogeneity and lipid infiltration was confirmed by Angio-CT (Figure 1).
Due to patient critical state, with protombine time prolongation and hypoglycemia she was transferred to intermediate care unit where she received fresh frozen plasma, intravenous fluids with glucose and vitamin K. Because of the high risk of hepatic failure the patient was then transferred to intensive unit care (ICU) 48 h after admission. It was performed a liver biopsy that revealed hepatocyte microesteatosis with centrilobular hepatocellular ballooning which confirmed the diagnosis of AFLP.
During the ICU stay the patient status improved gradually. Liver enzymes normalized 30 days after admission and there was a total recover of hepatic function with no need for liver transplantation. The newborn presented with perinatal hypoxic-ischemic encephalopathy grade I and hipotonia. She had stayed at neonatal NICU for 15 days and was discharged with follow-up at paediatric consultation. The newborn metabolic disease screening, that includes LCHAD mutation, was negative.
Discussion
Liver disease in pregnancy is a challenge for obstetricians. Pregnancy is associated with physiologic changes at hepatic function but when there are abnormalities they should be investigated1,8. AFLP is a serious maternal liver disease unique to pregnancy usually diagnosed at third trimester4,5. It is more common in women with multiple pregnancies, male fetus and primigravidas, however this case occurred in a single pregnancy of a female fetus with a previous pregnancy and postpartum without complications1,2,4.
]]> Recent studies linked AFLP to an inherited defect at the mitochondrial beta-oxidation of fatty acids. Some affected women and fetus have LCHAD deficiency that predisposes the mother to this disorder2,8,9. All women with AFLP and their children should be tested for at least more common LCHAD mutations. AFLP may recur in subsequent pregnancies even if the genetic screening is negative2,8,9.The majority of the cases of AFLP are diagnosed during pregnancy, however sometimes they are not clear until the pregnancy is terminated4. At this case report the patient had a nonspecific postpartum presentation making it difficult to establish the diagnosis. She presented clinical and laboratory findings that revealed hepatic dysfunction. The challenge was to define the etiology. There are many pregnancy related disorders that can occur with hepatic dysfunction like preclampsia, HELLP syndrome, intrahepatic colestasis, acute fatty liver, hepatotoxicity and hepatitis1,8,9.
Despite pre-eclampsia and cholestasis are more common conditions, in the presented case report, laboratory and imaging findings were in favour of AFPL. Moreover, blood pressure was normal during pregnancy and hospital admission and there wasn't proteinuria or any pre-eclampsia symptoms. At this case we verified that viral hepatitis screening was negative. There was not any drugs consumption during pregnancy8,9. Ultrasound and TC scan excluded hepatic infarct, thrombosis, or cholestasis and suggested hepatic fatty infiltration. AFLP and HELLP syndrome have some common laboratory findings but in AFLP there is more significant hepatic impairment particularly hypoglycaemia and marked coagulopathy. Our patient had normal hemoglobin and haptoglobin values and only slightly decreased platelets, which ruled out HELLP sydrome 1,10-12.
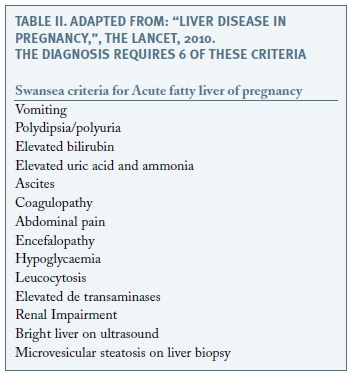
Based on clinical, laboratory and ultrasound findings the AFLP diagnosis was proposed as a diagnosis of exclusion. It was confirmed by liver biopsy6,9,11. However it is not always necessary to realize this invasive test. The Swansea diagnostic criteria can be an alternative to establish the diagnosis (Table II)1,5,8.
There are an increasing number of case reports at the literature that describe that suspicious or confirmed cases of AFLP are obstetric emergencies and should be treated with prompt termination of pregnancy3,5,8. When the diagnosis is established during pregnancy the risks of fetal distress and death are high, so continuous fetal monitoring and delivery is mandatory regardless of gestational age3-5. At some cases there can be fetal compromise without a clinical decompesation of the mother. At this specific case we didn´t find any other reason for the alterations in continue cardiotocography so it was an early manifestation of the maternal disorder.
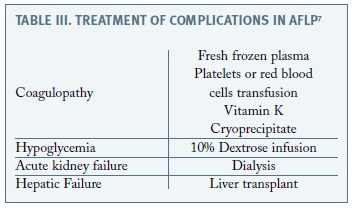
The route of delivery depends on maternal and fetal status, if possible vaginal birth and labour induction should be preferred 3,7. In this case the diagnosis of AFLP was outlined after delivery and adequate maternal surveillance and supportive therapy was promptly established avoiding liver transplantation. Maternal stabilization required glucose infusion, vitamin K and fresh frozen plasma (Table III)4,5-7.
]]>
Acute fatty liver is a serious pregnancy disorder with significant maternal and neonatal consequences. This case report reinforces the importance of prompt diagnosis and supportive therapy to improve the outcome and reduce maternal and neonatal mortality1,3,6.
REFERENCES
1. Ahmed K, Almashhrawi A, Rahman R, Hammoud G, Ibdah J. Liver diseases in pregnancy: Diseases unique to pregnancy. World J Gastroenterol 2013; 19:7639-7646. [ Links ]
2. Ibdah J. Acute fatty liver of pregnancy: An update on pathogenesis and clinical implications. World J Gastroenterol 2006; 12:7397-7404. [ Links ]
3. Ko H, Yoshida E. Acute fatty liver of pregnancy. Can J Gastroenterol 2006; 20: 25-30. [ Links ]
4. Sinha P, Kyle P, Gubbala P. Acute Fatty Liver of Pregnancy - A Review. The Internet Journal of Gynecology and Obstetrics. 2009; 13:1-5. [ Links ]
5. Dwivedi S, Runmei M. Retrospective Study of Seven Cases with Acute Fatty Liver of Pregnancy. ISRN Obstet Gynecol 2013; 3:1-7. [ Links ]
6. Riyami N, Al-Harthy A, Zia F. Atypical Case of Acute Fatty Liver of Pregnancy. Sultan Qaboos Univ Med J 2011; 11:507-510. [ Links ]
7. Lee R, Tran T. Acute fatty liver of pregnancy. uptodate 2016. [ Links ]
8. Joshi D, James A, Quaglia A, Westbrook R, Heneghan M. Liver disease in pregnancy. Lancet 2010; 375: 594-605. [ Links ]
9. Kondrackienė J, Kupčinskas L. Liver diseases unique to pregnancy. Medicina (Kaunas) 2008; 44:337-345. [ Links ]
10. Oliveira C, Moreira A, Baima J, Franzoni L, Lima T, Yamashiro F,Coelho K, Sassaki L, Caramori C, Romeiro F,Silva G. Acute fatty liver of pregnancy associated with severe acute pancreatitis: A case report. World J Hepatology 2014; 6: 527-531. [ Links ]
11. Kobayashi T, Minami S, Mitani A. Tanizaki Y, Booka M, Okutani T, Yamaguchi S, Ino K. Acute fatty liver of pregnancy associated with fetal mitochondrial trifunctional protein deficiency. J Obstet Gynaecol Res 2015; 41:799-802. [ Links ]
12. Nelson D, Yost N, Cunningham F. Hemostatic dysfunction with acute fatty liver of pregnancy. Obstet Gynecol. 2014; 124: 40-46. [ Links ]
]]> Endereço para correspondência | Dirección para correspondencia | Correspondence
Fernanda Vilela
Centro Hospitalar do Algarve - Unidade de Faro
E-mail: fernandavilela17@gmail.com
Recebido em: 26/09/2016
Aceite para publicação: 30/05/2017
]]>