Recurrent acute pancreatitis in pregnancy
Pancreatite aguda recorrente na gravidez
Nadia Charepe1, Ana Sofia Rodrigues1,Ana Catarina Massa2, Maria José Alves2
Maternidade Dr. Alfredo da Costa
1. Interna de Ginecologia e Obstetrícia
2. Especialista de Ginecologia e Obstetrícia
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
]]> Introduction: During pregnancy pancreatitis is a rare and diagnosis is difficult. Cholelithiasis is the most frequent risk factor.Case report: A 26-year-old pregnant woman with abdominal pain, vomiting and low-grade fever. Hyperamylasemia and cholelithiasis was found and pancreatitis diagnosis was made. A second episode of acute pancreatitis was observed and treated with medical therapy. There was no foetal or neonatal complications. In puerperium a third pancreatitis occurred, a laparoscopic cholecystectomy was performed.
Discussion: Diagnosis of acute pancreatitis in pregnancy is challenging and it may have serious maternal-fetal implications. Recurrent pattern should be taken into account when choosing the best treatment.
Keywords: Recurrent acute pancreatitis; Pregnancy; Cholelithiasis.
Introduction
Acute pancreatitis is a rare condition during pregnancy with an incidence of 1 in 1000 to 10000 deliveries1. Its diagnosis is challenging since abdominal pain in pregnancy may have several etiologies. Risk factors for acute pancreatitis include cholelithiasis that represents about 70% of all cases1 hypertriglyceridemia, obesity and others. During pregnancy there is usually a worsening of lithiasic disease due to the lithogenic effect of estrogen and progesterone specially in the third trimester of pregnancy. Therefore, acute pancreatitis caused by cholelithiasis is more frequent as gestational age increases7. Pregnancy-induced hypertension contributes to microvasculature alterations and ischemic episodes in splanchnic circulation which may lead to acute pancreatitis1. A high level of suspicion is needed to make the diagnosis and, if absent or delayed, there is a high maternal-fetal morbidity and mortality rate. Abdominal pain is the main symptom but it can be related to other obstetric disorders such as labor, preeclampsia, HELLP syndrome (hemolysis, elevated liver enzyme levels, and low platelet levels), fatty liver of pregnancy, placental abruptio, uterine rupture, chorioamnionitis or medical disorders, such as appendicitis, pneumonia and gastroesophageal reflux disease. Some of these conditions might present simultaneously. Nevertheless, the diagnostic criteria are the same as for the non-pregnant population. Abdominal pain that radiates to the back, nausea and vomiting, anorexia, low-grade fever and tachycardia are the most frequent signs and symptoms. The presence of at least two of the Atlanta criteria is needed to make the diagnosis. The criteria are (revised classification): (a) abdominal pain suggestive of pancreatitis (epigastric pain often radiating to the back); (b) amylase/lipase levels three or more times normal; (c) characteristic findings on computed tomography scan, magnetic resonance imaging, or abdominal ultrasound3. The abdominal ultrasound might reveal the presence of bile sludge or gallstones. The best predictor factor of severity is the C reactive protein (CRP) (>150 mg/dL). There are several scoring systems such as Ranson score that helps to identify pancreatitis severity allowing to allocate patient to the best setting of care13. Concerning treatment, during pregnancy there is a preference for conservative over surgical treatment2. The latter is kept for complications such as abscess, gastrointestinal perforation, infected abdominal effusion or failure to improve after medical therapy2. An endoscopic retrograde cholangiopancreatography (ERCP) to remove bile ducts stones can also be considered. Pregnancy termination is indicated at term, if clinical deterioration after 48 hours of medical therapy or severe pancreatitis. In the post-partum there is a decline in the incidence of this condition because the bile composition and gallbladder function return to normal. It is expected that bile sludge resolves spontaneously (in 39% of cases) and gallbladder stones less than 10 mm tend to disappear2.
Case report
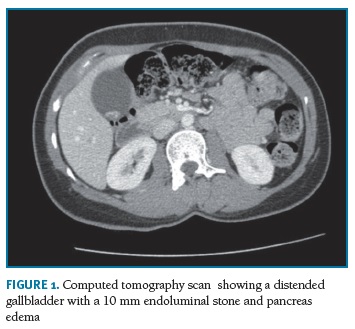
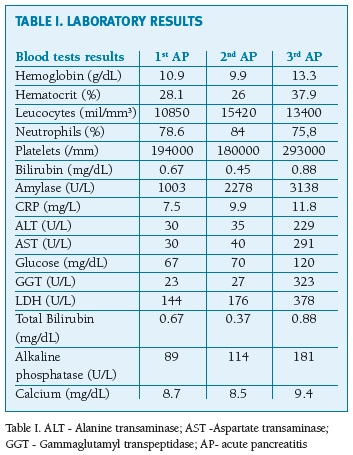
A 26-year-old healthy pregnant woman, from Bangladesh, with an obstetric history of a vaginal delivery in 2015 presented to our emergency room. She had been doing her antenatal appointments with her family doctor and during the first trimester, she had hyperemesis gravidarum (treated with metoclopramide and latter with ondansetron) and iron deficiency anemia. There was no alcohol or drugs consumption. She was admitted at 20 weeks of gestation with nausea and vomiting related to epigastric pain that radiated to the back during the previous month. Before pregnancy she had episodes of epigastric pain after intake of fatty food. No hypertensive symptoms were present. Physical examination revealed a low body mass index (18 Kg/m2) and loss of 6 Kg in the last month. She was pale but with no jaundice with low-grade fever (37.6º C) and pain in the epigastric region at abdominal examination. There was no hypertension or peripheral edema. During the previous month, abdominal pain was the reason for multiple medical appointments with only symptomatic measures taken in place. An obstetric ultrasound was performed showing an active fetus. Laboratory evaluation revealed an amylase 1003 U/L (normal reference value 0-160 U/L) and CRP 7,5 mg/L (normal reference value < 5 mg/L) (see Table I). After the diagnosis of acute pancreatitis, an abdominal ultrasound was performed that exhibited gallbladder microlithiasis with no bile ducts ectasia, pancreatic body or tail edema. She was admitted to the surgical ward and medical treatment was started (analgesia). Over the next days, symptoms improved and blood tests returned to normal. She was discharged 5 days later, asymptomatic. She returned to the emergency room 2 weeks later with similar symptoms; blood test results were abnormal (see Table I). An abdominal ultrasound showed again microlithiasis with no bile ducts ectasia, pancreatic body or tail edema. A new diagnosis of acute pancreatitis was assumed and treated with conservative measures. Obstetric evaluation showed no complications. The remaining pregnancy was uneventful. She had a vacuum-assisted vaginal delivery at term; the newborn weighted 3005 gr and had an Apgar Score of 10/10. In the post-partum she had a third acute pancreatitis and a computed tomography scan was performed revealing a distended gallbladder with a 10 mm endoluminal stone; no bile ducts ectasia but pancreas edema was present (Figure 1). The Ranson criteria score was 0 (1st and 2nd episodes and 1 at 3rd episode). A laparoscopic cholecystectomy was proposed.
]]>
Discussion
Recurrent acute pancreatitis in pregnancy is rare but can be responsible for a high maternal-fetal morbidity such as multiorgan failure, sepsis and preterm labor or fetal hypoxia and even death2. A high level of clinical suspicion is essential because a delayed diagnosis can lead to a severe deterioration and unintended morbidity and mortality. This case report illustrates that it is possible to have more than one condition simultaneously during pregnancy that can be responsible for similar symptoms. Hyperemesis gravidarum, present since the first trimester, was the confounding condition in this case and for this reason diagnosis was delayed leading to a prolonged presentation of symptoms with weight loss and several hospitalizations. Differential diagnosis with other entities includes HELLP syndrome and gastroesophagic reflux. HELLP syndrome is a life-threatening pregnancy complication and it can be difficult to diagnose, especially when high blood pressure and protein in the urine are absent and gastroesophagic reflux is very frequent in pregnancy.
Ultrasound can be used as an early and elementary prognostic indicator for severity of pancreatitis, if we can observe acute fluid collection, but also important in understanding the etiology. A Ranson score of 0/1 predicts that complications and mortality will be negligible, as seen in this case report13.
Concerning treatment, there is still some uncertainty, whether a laparoscopic cholecystectomy should be performed, an ERCP or even a conservative approach. For some authors, management of acute pancreatitis should be individualized based on gestational age, leaving conservative treatment for the first trimester, laparoscopic surgery for the second and ERCP or conservative management for third trimester10. Recent literature has showed that laparoscopic cholecystectomy is safe during any trimester of pregnancy, contradicting previous knowledge that was only safe during the second trimester. If symptomatic gallstones disease is present during pregnancy, postponing surgery to postpartum period can lead to complications for both mother and fetus8. Laparoscopic surgery during pregnancy has several advantages when compared with abdominal laparotomy such as decreased postoperative pain, fetal respiratory depression, maternal hypoventilation, uterus manipulation and thromboembolic complications.
During this procedure, special care should be put in place. Patient positioning, port placement taking into account the fundal height, insufflation pressure of a maximum 10-15 mmHg, monitoring level of CO2 with capnography and venous thromboembolic prophylaxis. Tocolytics can be considered perioperatively if preterm labor is iminent 8. ERCP is an option but there are some risks such as premature birth, spontaneous abortion, infection, perforation and bleeding; however these risks are low7. It is important to consider this approach if a strong indication is present such as choledocholithiasis. The procedure has to be adjusted for pregnant population with proper shielding, patient positioning in left lateral decubitus and minimize procedure time. Fluoroscopy during the first trimester should be avoided, even though the fetus can be shielded, due to the risk of cancer in childhood. There is some controversy if an endoscopic sphincterotomy is sufficient to prevent recurrency of acute pancreatitis in pregnant population with gallstones or even microlithiasis postponing laparoscopic cholecystectomy in postpartum period or not even considering at all9. It seems that laparoscopic cholecystectomy in puerperium or before another subsequent pregnancy should be performed, so that no more episodes of pancreatitis occur. There are few studies regarding acute pancreatitis in pregnancy. In 2008, Eddy et al published a 10-year multicentre retrospective study with 101 acute pancreatitis during pregnancy due to lithiasis that showed a tendency for a reduction of preterm labor and recurrence of pancreatitis if initial treatment was surgical (although these results were not statistically relevant)5. In conclusion, acute pancreatitis during pregnancy poses a serious threat to the safety of the mother and fetus. For this reason, additional multicentric studies are necessary to understand if a more invasive approach will reduce the number of recurrent episodes during pregnancy and post-partum and improve maternal-fetal outcomes.
]]> REFERENCES
1. Igbinosa O., Poddar S., Pitchumoni C. Pregnancy associated pancreatitis revisited. J.CLINRE 2013; 37: 177-181. [ Links ]
2. Srikumar S., Nair S., Reghunath R., Raj S., Radhamany K. Acute pancreatitis in pregnancy: 5- year experience from a multidisciplinary centre. IJRCOG 2018;7(2):546-551. [ Links ]
3. Thoeni R. The Revised Atlanta Classification of Acute Pancreatitis: Its Importance for the Radiologist and Its Effect on Treatment in: Radiology. RSNA 2012; 262(3):751-764. [ Links ]
4. Juneja S., Gupta S., Virk S., Tandon P., Bindal V. Acute pancreatitis in pregnancy: A treatment paradigm based on our hospital experience, Int J Appl Basic Med Res. 2013; 3(2): 122-125. [ Links ]
5. Eddy J., Gideonsen M., Song J., Grobman W., O’Halloran P. Pancreatitis in Pregnancy: a 10 year retrospective of 15 Midwest hospitals. Obstet Gynecol. 2008; 112(5): 1075-1081.
]]>6. Mali P. Pancreatitis in pregnancy: etiology, diagnosis, treatment, and outcomes. HBPD 2016; 15(4): 434-438. [ Links ]
7. Inamdar S, Berzin TM, Sejpal DV, Pleskow DK, Chuttani R, Sawhney MS, Trindade AJ. Pregnancy is a Risk Factor for Pancreatitis After Endoscopic Retrograde Cholangiopancreatography in a National Cohort Study. Clin Gastroenterol Hepatol. 2016; 14 (1):107-114. [ Links ]
8. Pearl J., Price R., Tonkin A., Richardson W., Stefanidis D., Guidelines for the use of laparoscopy during pregnancy. SAGES 2017; 1-29.
9. Barthel JS, Chowdhury T, Miedema BW. Endoscopic sphincterotomy for the treatment of gallstone pancreatitis during pregnancy. Surg Endosc. 1998; 12 (5):394-349. [ Links ]
10. Ducarme G, Maire F, Chatel P, Luton D., Hammel P. Acute pancreatitis during pregnancy: a review. J Perinatol 2014; 34:87-94. [ Links ]
12. Arafata M., Ghaffara I., El- Hussainya A., Alkhalika M., Ahmadc M., Mostafabneous T. Safety and feasibility of laparoscopic cholecystectomy during pregnancy. J. ASMR 2016; 9-13
]]> 13. Ruan GJ, Mukherjee S. Ranson Criteria StatPearls Publishing 2019; 1-6
Endereço para correspondência | Dirección para correspondencia | Correspondence
Nadia Charepe
Maternidade Alfredo da Costa
Lisboa, Portugal
E-mail: nadiacharepe@gmail.com
Recebido em: 07/02/2019
Aceite para publicação: 30/04/2019
]]>