Bilateral persistent sciatic artery: a case report of a rare variant with clinical implications
Artéria ciática persistente bilateral: variante rara clinicamente significativa
Tiago André Moura Rodrigues1, Madalena Ramalho1, Tiago Ferreira2, Augusto Ministro2, João Leitão1
1Department of Radiology, Hospital de Santa Maria, Lisbon
2Department of Angiology and Vascular Surgery, Hospital de Santa Maria, Lisbon
Autor para correspondência
ABSTRACT
]]> Although rare, the persistence of a sciatic artery is a clinically significant vascular variant, since it is often associated with complications such as aneurysm formation, thrombosis and ischaemia. We present the case of a patient with signs of subacute ischaemia on the right lower limb and a pulsatile mass in the right inferior gluteal region. CT angiography revealed a bilateral persistent sciatic artery (PSA) complicated by aneurysm formation and embolization of distal popliteal artery. Treatment included a femoro-popliteal bypass, ligation of the popliteal artery above the anastomosis and embolization of the aneurysmal lesion.Keywords: Persistent sciatic artery, anatomic variants, aneurysm, lower extremity, CT-Angiography
.
RESUMO
Embora rara, a persistência da artéria ciática é uma variante anatómica com significado clínico, uma vez que está frequentemente associada a complicações como formação de aneurismas, trombose e isquemia distal. Apresentamos o caso de um doente com sinais de isquemia subaguda do membro inferior direito e uma massa pulsátil na vertente inferior da região glútea homolateral. A angiografia por tomografia computorizada demonstrou a existência de uma artéria ciática persistente bilateral, à direita complicada por aneurisma parcialmente trombosado e embolização distal para a artéria poplítea. O tratamento cirúrgico incluiu a realização de um bypass femoro-poplíteu, a laqueação da artéria poplítea acima da anastomose e a embolização da lesão aneurismática.
Palavras-chave: Artéria ciática persistente, variante anatómica, aneurisma, membro inferior, Angio-TC
INTRODUCTION
During early embryonic life, sciatic arteries are the major arterial structures providing blood to lower limb buds. Normally, they progressively regress and their function is completely replaced by femoral arteries at around the 3rd month of gestation(1). However, in an estimated 0,05% of population(2), the sciatic artery does not completely involute, and therefore becomes persistent. The persistent sciatic artery can be complete or incomplete, unilateral or bilateral and co-exist with a fully or underdeveloped superficial femoral artery(3). Despite its rarity, identification of PSA has clinical importance, because it is frequently associated with complications such as aneurysmal lesions, thrombosis and variable degrees of distal ischaemia(4). Failure to identify a PSA can also lead to poor surgical planning and management.
]]> REPORT
We present the case of a 76 year-old man with chronic right lower limb claudication, which had progressed to rest pain during the previous 2 weeks. No episode of trauma and no history of smoking, hypertension or diabetes were noted.
Physical examination was remarkable for a pulsatile mass at the right inferior gluteal region. The right extremity was cold, with slow capillary refill time. Both femoral and popliteal pulses were palpable, but pedal and posterior tibial pulses were absent.
The left extremity showed signs of chronic vascular disease, but was asymptomatic.
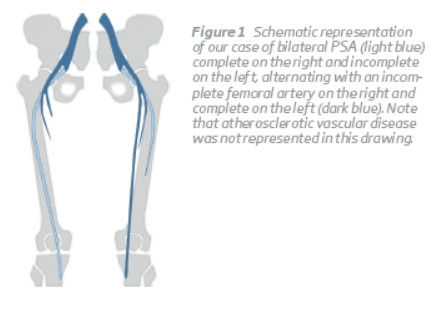
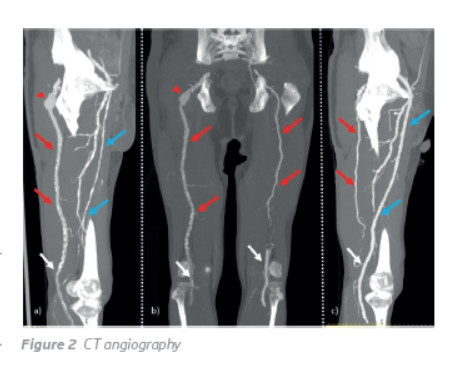
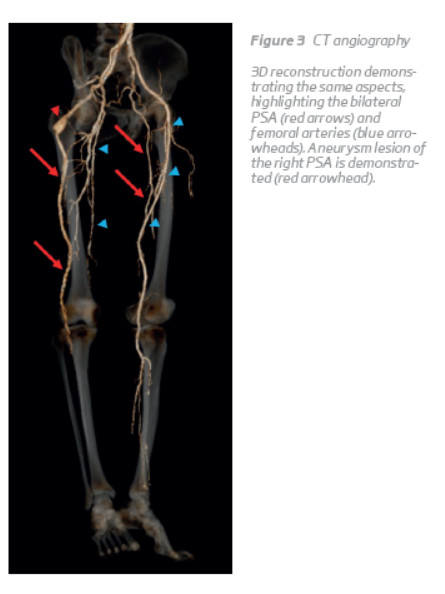
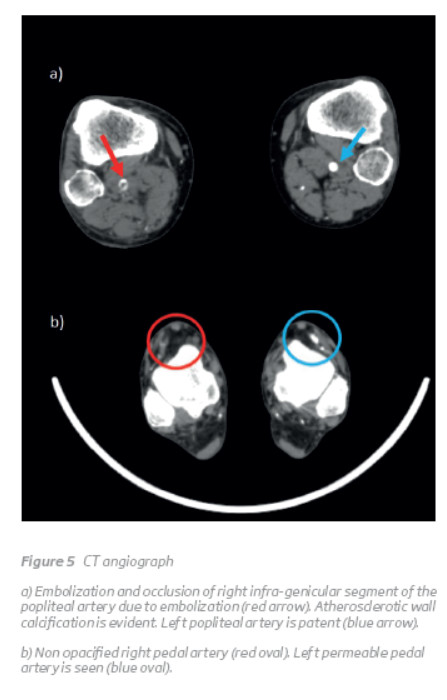
CT angiography of the abdominal aorta and lower limbs revealed a bilateral persistent sciatic artery, with complete persistence on the right side and incomplete on the left. As opposed to PSAs, the superficial femoral artery was incomplete on the right side and complete on the left (Figure 1, 2 and 3). Furthermore, a 4.3-cm partially thrombosed saccular aneurysm was identified in the retroischiatic segment of the right PSA (Figure 4), and an occluded segment due to embolization was demonstrated in the infragenicular popliteal artery (Figure 5). No pedal flow was seen and only a faint opacification of the distal segments of the peroneal artery was present.
 ]]>
]]>

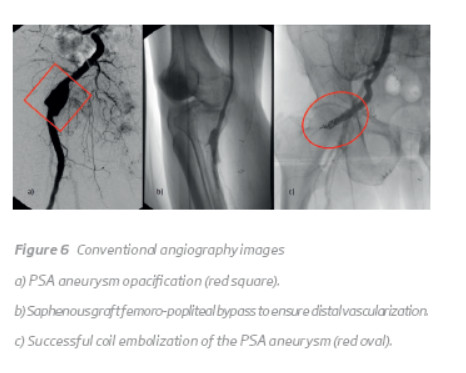
]]> The patient underwent a femoro-popliteal bypass with great saphenous vein graft along with proximal ligation of the popliteal artery above the anastomosis. Coil embolization of the PSA aneurysm was performed on a second surgical procedure (Figure 6). The patient had no post-operative complications and vascularization to right leg and foot was re-established.
DISCUSSION
We presented a rare case of bilateral and asymmetric PSA (complete on the right and incomplete on the left). Interestingly, femoral and PSA arteries development alternated in an inverse manner, as they establish dominant blood flow to the extremities. According to the classification of PSA by Pillet et al.(5), this would represent a type 2a persistence on the right and a type 3 persistence on the left. To our knowledge, this is the fifth case of combined-type PSA (complete on the right and incomplete on the left) published in literature(1).
Diagnosis of PSA and related complications is made on clinical grounds and imaging findings. We would like to point out that in our particular case, Cowie's sign (diminished or absence of femoral pulse in combination with palpable popliteal pulse) was absent, since there was still an incompletely developed femoral artery on the right. Doppler ultrasound can provide valuable initial information about the extent and severity of peripheral vascular disease, although CT angiography is usually necessary to confirm the diagnosis of PSA, evaluate possible complications and plan surgical approach.
Although not fully understood, some authors suggest that the high rate of aneurysm formation in PSA is due to its anatomic location, which favours overstretching during flexion of the hip joint and repeated trauma against the sacrospinal ligament, piriform muscle and hip(2,6).
There are different therapeutic options, but embolization of PSA aneurysm is often preferred over exclusion, since the latter is associated with sciatic nerve injuries. Another factor to take into consideration is the type of PSA present, because an additional bypass may be needed in the scenario of an incompletely developed femoral artery, as in our case.
]]> REFERENCES
M. van Hooft, C. J. Zeebregts, S. M. M. van Sterkenburg, W. R. de Vries, and M. M. P. J. Reijnen, “The Persistent Sciatic Artery,” Eur. J. Vasc. Endovasc. Surg., vol. 37, no. 5, pp. 585–591, 2009. [ Links ]
Cavallo Marincola, A. Napoli, M. Anzidei, E. Marotta, F. Boni, G. Cartocci, L. Bertaccini, V. Noce, M. Antonietta Pacilé, and C. Catalano, “Persistence of the sciatic artery: a case report of a combined (complete and incomplete) type causing leg ischemia.,” Case Rep. Vasc. Med., vol. 2012, p. 196798, 2012. [ Links ]
Gauffre, P. Lasjaunias, and M. Zerah, “Sciatic artery: a case, review of literature and attempt of systemization,” Surg. Radiol. Anat., vol. 16, no. 1, pp. 105–109, 1994. [ Links ]
Graf, B. Keyashian, A. Brown, S. M. Tutton, and C. J. Lee, “A hybrid approach for the treatment of persistent sciatic artery aneurysms,” J. Vasc. Surg. Cases Innov. Tech., vol. 2, no. 4, pp. 174–177, 2016. [ Links ]
J. Pillet J, Cronier P, Mercier Ph, “The ischio popliteal arterial trunk: a report of two cases.,” Anat Clin, vol. 3, p. 329e31, 1982. [ Links ]
K. Brantley, E. E. Rigdon, and S. Raju, “Persistent sciatic artery: Embryology, pathology, and treatment,” J. Vasc. Surg., vol. 18, no. 2, pp. 242–248, 1993. [ Links ]
Correio eletrónico: tiagomourarodrigues@gmail.com (T. Rodrigues).
Recebido a 2017-03-11;
Aceite a 25-10-2017;
]]>