Pancreatic Mucinous Cystadenoma Mimicking Intraductal Papillary Mucinous Neoplasm
Cistadenoma Mucinoso Mimetizando Neoplasia Mucinosa Papilar Intraductal do Pâncreas
Susana Marques, Joana Carmo, Miguel Bispo
Department of Gastroenterology, Centro Hospitalar Lisboa Ocidental, Lisbon, Portugal
* Corresponding author.
Keywords: Acute pancreatitis, Ultrasound endoscopy
]]> Palavras-Chave: Pancreatite aguda, Ultrassonografia endoscópica
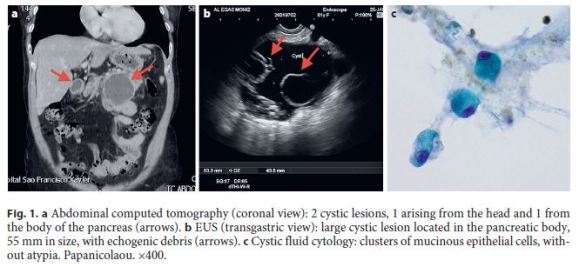
A 61-year-old female patient presented with epigastric pain radiating to the back for the previous 2 days. Physical examination revealed diffuse abdominal pain with epigastric tenderness. Laboratory results showed elevated lipase (2,946 UI/L). At this point, the diagnosis of acute pancreatitis (AP) was established. Abdominal ultrasonography and computed tomography revealed cystic pancreatic lesions arising from the head, body, and tail of the pancreas, ranging from 1 to 5.5 cm (Fig. 1a), with no evidence favoring a biliary cause for the AP. The patient was kept on n.p.o. and i.v. vigorous hydration and pain medication were provided. The clinical evolution was favorable and the patient was discharged after a 3-day hospital stay. Two weeks after discharge, an endoscopic ultrasound (EUS) was performed and showed 4 pancreatic cystic lesions, 2 arising from the head, 1 from the body, and 1 from the tail, ranging from 5 to 55 mm and apparently all communicating with the main pancreatic duct, which was not dilated. Echogenic debris were observed inside the largest cystic lesion (Fig. 1b). A transgastric EUS-fine needle aspiration of the largest cyst was performed and revealed high amylase (>48,000 UI/L) and CEA (291 ng/mL) levels and clusters of mucinous epithelial cells, without atypia (Fig. 1c). All imaging, laboratory, and pathological findings were consistent with the diagnosis of a multifocal branch duct intraductal papillary mucinous neoplasm (IPMN). Due to the size of the largest cyst (≥3 cm) and the clinical presentation (pancreatitis), both worrisome features [1], the patient underwent a distal pancreatectomy. Unexpectedly, the final pathology diagnosis revealed a mucinous cystadenoma of the pancreatic body and tail with focal high-grade dysplasia. The patient remains under surveillance for the other cysts, with morphologic characteristics of branch duct IPMN.
IPMN and mucinous cystic neoplasia (MCN) are two different types of mucinous cystic pancreatic neoplasms and may present as AP due to obstruction of the main pancreatic duct by thick mucus secretion. In both lesions, EUS-guided cyst aspirate is typically viscous and characterized by the presence of columnar or cuboidal mucinous epithelial cells in pathology and high CEA levels in chemistry analysis. The presence of an ovarian-like stroma is a unique pathological feature of MCN. IPMN has no gender predilection, is more common in the pancreatic head, and may be multifocal. On the contrary, MCN occurs almost exclusively in women (98%) and is usually a single lesion located in the body and tail of the pancreas (95%). Because IPMN communicates with the main pancreatic duct and MCN typically does not, the amylase fluid level is expected to be high in IPMN and within the normal range in MCN [1]. Despite distinct demographic, imaging, and laboratory features, distinguishing between an IPMN and a MCN is sometimes difficult. Up to 7% of MCNs communicate with the pancreatic duct due to the development of a fistula between the cyst and the pancreatic duct. In this very rare situation, an MCN may have high amylase level and be therefore misdiagnosed as an IPMN, such as happened in this case [2].
References
1 Tanaka M, Castillo CF, Adsay V, Chari S, Falconi M, Jang JY, et al: International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 2012;12:183197. [ Links ]
]]>2 Morel A, Marteau V, Chambon E, Gayet B, Zins M: Pancreatic mucinous cystadenoma communicating with the main pancreatic duct on MRI. BR J Radiol 2009;82:e243e245. [ Links ]
Statement of Ethics
This study did not require informed consent nor review/approval by the appropriate ethics committee.
Disclosure Statement
The authors have no conflicts of interest to declare.
* Corresponding author.
Dr. Susana Marques
]]> Department of Gastroenterology, Centro Hospitalar Lisboa OcidentalRua da Junqueira 126
PT1349-019 Lisbon (Portugal)
E-Mail xsusanamarx@gmail.com
Received: May 18, 2017; Accepted after revision: August 22, 2017
]]>