Mixed Adenoneuroendocrine Tumor of the Rectum in an Ulcerative Colitis Patient
Tumor adenoneuroendócrino misto do reto num doente com colite ulcerosa
Rui Gaspara, João Santos-Antunesa, Margarida Marquesa, Rodrigo Liberala, Daniel Melob, Pedro Pereirab, Susana Lopesa, Guilherme Macedoa
aGastroenterology Department, Centro Hospitalar São João, Porto, Portugal; bDepartment of Pathology, Centro Hospitalar São João, Porto, Portugal
* Corresponding author.
ABSTRACT
]]> Patients with inflammatory bowel disease present a higher risk of colorectal cancer, especially patients with a high degree of disease activity. Although rare, carcinoid tumors can also be associated with inflammatory bowel disease. Mixed adenoneuroendocrine tumor is defined as a neoplasm with dual differentiation (neuroendocrine and adenoma) with each component accounting for at least 30% of the tumor. We present a case of a mixed adenoneuroendocrine tumor in a patient with inflammatory bowel disease.Keywords: Adenoneuroendocrine carcinoma, Ulcerative colitis, Endoscopic submucosal dissection
RESUMO
Doentes com doença inflamatória intestinal apresentam um risco elevado de carcinoma colo-retal, principalmente quando apresentam uma elevada atividade da doença. Apesar de raros, os tumores carcinoides também se podem associar a doença inflamatória intestinal. O tumor adenoneuroendócrino misto define-se como uma neoplasia com diferenciação dupla (neuroendócrino e adenoma), sendo cada componente responsável por pelo menos 30% do tumor. Apresentamos um caso de um tumor adenoneuroendócrino num doente com doença inflamatória intestinal.
Palavras-Chave: Carcinoma adenoneuroendócrino, Colite ulcerosa, Disseção endoscópica da submucosa
Clinical Case
We present the case of a 66-year-old male patient with a 30-year history of ulcerative colitis (E3). He was asymptomatic under mesalazine 3 g/day, and the surveillance colonoscopy performed outside the hospital the year before, with fair quality of bowel preparation, was unremarkable.
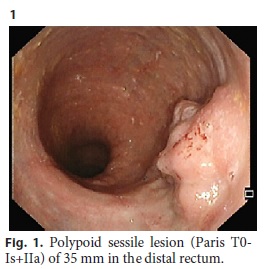
In our hospital, his annual colonoscopy was performed and showed a polypoid sessile lesion (Paris classification T0-Is+IIa) of 35 mm in the distal rectum with unclear margins (Fig. 1). The surrounding mucosa showed marked erythema, absent vascular pattern and erosions. Evaluation with high-definition endoscopy, chromoendoscopy with indigo, and narrow band imaging showed no suspicion of malignancy. The biopsies revealed an adenomatous lesion with low-grade dysplasia. Laboratory data and tumor markers were unremarkable.
]]>
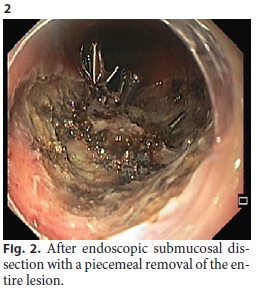
It was decided to perform an endoscopic submucosal dissection due to the high probability of severe submucosal fibrosis and the impossibility of en bloc resection with endoscopic mucosal resection. Endoscopic submucosal dissection was performed under deep sedation with propofol, with dual knife, and took 5 h. The procedure was difficult due to severe fibrosis of the submucosa, with poor lifting and severe mucosal friability. A hemoclip was performed in a large vessel for bleeding prophylaxis and on another site due to superficial muscular injury. The entire lesion was removed in 2 fragments (2.2 × 1.7 × 1 and 1 × 1.3 × 0.5 cm), and the patient was discharged on the following day (Fig. 2).
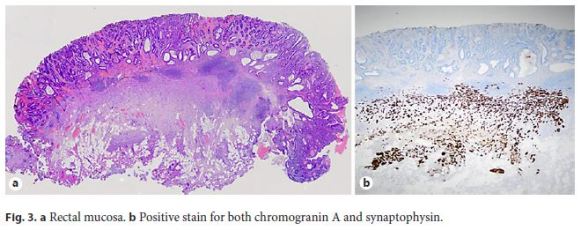
The histopathology of the specimen revealed a tubular adenoma with high-grade dysplasia with focal neuroendocrine differentiation. The neuroendocrine features were found in the marginal area of the tumor (representing more than 30% of the total size), which stained positive for both chromogranin A and synaptophysin, with a Ki67 index of 5.2% (Fig. 3). The resection was not complete, as the deep margin was involved with the neuroendocrine tumor. It was decided to perform an OctreoScan that raised the suspicion of a lymph node metastasis in the mesenteric superior artery. On the multidisciplinary group clinic appointment, it was decided to perform an abdominopelvic computed tomography due to suspicion of metastatic disease, which was unremarkable. Due to the suspicion on the OctreoScan, the patient was started on chemotherapy with lanreotide. At the 1-year follow-up, the revaluation colonoscopy did not show evidence of recurrent disease.
Patients with ulcerative colitis present a higher risk of dysplasia and colorectal cancer. A family history of colon cancer, high extent of colitis, duration of more than 810 years of the disease, primary sclerosing cholangitis as well as active inflammation and a history of dysplasia are risk factors for colorectal cancer in patients with ulcerative colitis [1]. Carcinoid tumors and neuroendocrine neoplasms other than carcinoids can also be associated with inflammatory bowel disease because of the increased number of neuroendocrine cells found in inflamed mucosa [2]. However, the association of neuroendocrine tumors with inflammatory bowel disease is extremely rare, with only 13 reports from 1980 to 2015. It has been hypothesized that the development of neuroendocrine tumors in inflammatory bowel disease patients may result from chronic inflammation of the colonic mucosa, which may cause pancellular damage, including neuroendocrine cells, and from distant secretion of cytokines of systemic mediators [3].
Mixed adenoneuroendocrine tumor (MANET) is defined as a neoplasm with dual differentiation (neuroendocrine and adenoma) with each component accounting for at least 30% of the tumor [4, 5]. Although having a better prognosis than mixed adenoneuroendocrine carcinoma, MANETs can also metastasize, requiring a more complex management [5].
]]> In conclusion, MANET is a rare entity that can present in patients with inflammatory bowel disease, and, despite the mild to moderate nuclear atypia and low number of mitoses, MANET can metastasize.
References
1 Beaugerie L, Itzkowitz SH: Cancers complicating inflammatory bowel disease. N Engl J Med 2015;372:14411452. [ Links ]
2 Grassia R, et al: Neuroendocrine carcinomas arising in ulcerative colitis: coincidences or possible correlations? World J Gastroenterol 2009;15:41934195. [ Links ]
3 Rifu K, et al: Sigmoid colon carcinoma with focal neuroendocrine differentiation associated with ulcerative colitis: a case report. Int J Surg Case Rep 2016;23:151156. [ Links ]
4 Watanabe J, et al: Clinicopathological and prognostic evaluations of mixed adenoneuroendocrine carcinoma of the colon and rectum: a case-matched study. Dis Colon Rectum 2016;59:11601167. [ Links ]
5 La Rosa S, et al: Mixed adenoneuroendocrine carcinomas (MANECs) of the gastrointestinal tract: an update. Cancers (Basel) 2012;4:1130. [ Links ]
Statement of Ethics
This study did not require informed consent nor review/approval by the appropriate ethics committee.
Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Sources
There were no funding sources.
]]>* Corresponding author.
Dr. Rui Gaspar
Department of Gastroenterology, Porto Medical School
Centro Hospitalar São João, Alameda Prof. Hernani Monteiro
PT4200-319 Porto (Portugal)
E-Mail ruilopesgaspar@gmail.com
Received: November 29, 2017; Accepted after revision: April 17, 2018
]]>