











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
Among different carpal bones, those placed at the proximal row are more prone to fracture.1 Trapezium fractures are rare, accounting for 0.4% of hand’s injuries2,3) and 3%-5% of carpal fractures.4-6
Due to the low prevalence and difficulty in diagnosing isolated trapezium fractures by routine imaging, high clinical suspicion, careful history taking, physical examination, and imaging interpretation are needed to avoid missing this diagnosis.1
A universal protocol for its treatment is lacking.7 Several treatment options have been described in the literature.3,6,7
In this paper, we report a case of a 54-year-old male patient with an isolated trapezium fracture following a motorcycle accident. It then further delineates its clinical and radiologic outcomes. Conservative treatment followed by progressive mobilization and strengthening resulted in union with excellent thumb function and no complications. The patient returned to his previous level of activity with an excellent outcome 2.5 months after the injury.
The aim of this report is to increase awareness regarding trapezium fractures, diagnostic tools and to share our treatment experience. It also illustrates a fracture’s pattern not mentioned on Walker’s classification.
Case report
A 54-year-old informatics engineer male patient presented to the Emergency Department (ED) on the same day following a motorcycle accident. Mechanism of trauma consisted of falling onto the hand with the extended wrist and the hand in radial deviation. He reported pain and swelling on the radial half of his left non-dominant hand.
On examination there was tenderness over the trapezium, base of first metacarpal and anatomical snuffbox.
Thumb motion was slightly painfully inhibited, the maximum pain being produced on marked opposition. His neuro-vascular status was intact. There were no signs of carpal instability. No skin lesions were evident. His past medical and family history, surgical and social history were unremarkable.
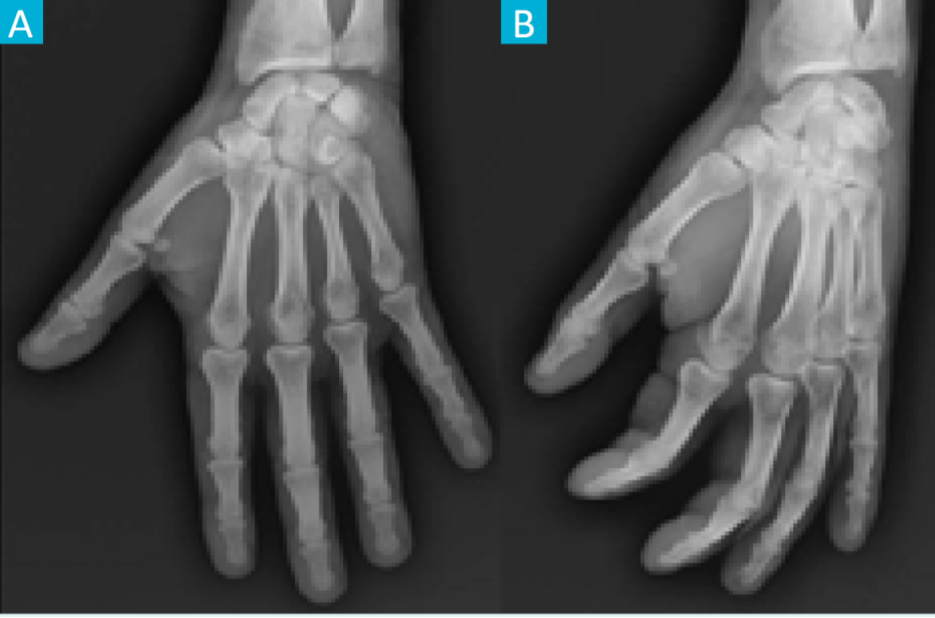
Figure 1: Left hand radiographs at presentation in anteroposterior (A) and oblique (B) projections. Both were inconclusive, showing no obvious fractures and intact trapeziometacarpal joint.
Plain radiographs of the left hand were inconclusive (Fig. 1). Because of the amount of pain and the suspiciousness of a carpal injury, a short-arm thumb spica was applied. Two days after, magnetic resonance imaging (MRI) indicated a fracture of the trapezium, with no associated lesions. Computed tomography scan (CT scan) was obtained to further characterize the anatomy of the fracture. It showed a minimally displaced small volar fragment, not mentioned on Walker’s classification (Fig. 2). Trapeziometacarpal congruence was evident, and all other carpal bones were intact. To our best knowledge, this fracture pattern has not been reported before.
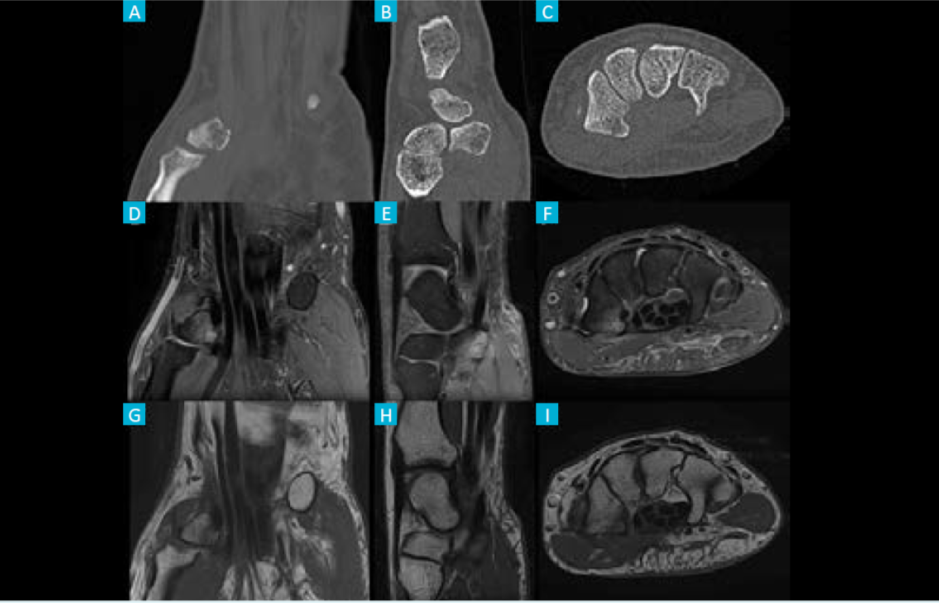
Figure 2: Left hand computed tomography scan (A - coronal, B - sagittal and C - axial views) and magnetic resonance imaging (D - coronal DP FS, E - sagittal DP FS, F - axial DP FS, G - coronal T1, H - sagittal T1 and I - axial T1) showing a non-displaced small volar fragment of the trapezium.
Fracture was non-displaced, so we decided to keep conservative treatment with a short-arm thumb spica.
Six weeks after the injury, the immobilization was removed, and the patient started physiotherapy to improve range of motion (ROM) and strength.
Two months following the injury, the patient regained a full range of unrestricted, painless thumb movements and full hand function (Fig. 3). There was no local tenderness.

Figure 3: Follow-up at 2 months, following conservative treatment with short-arm thumb spica for six weeks: range of motion of both hands.
The Grind test did not show any joint limitations or pain.
The patient reported satisfactory return to all his normal activities of daily living and returned to work with no limitations 2.5 months after the injury.
At the final follow up - 12 months after the injury - the outcome was excellent and symmetric to the non-injured side. The fracture healed with no complications.
His QuickDASH (disabilities of the arm, shoulder and hand) score was zero.
Discussion
Trapezium plays a major role in thumb’s function.4 The saddle shape of the trapeziometacarpal joint and its stabilizing ligaments have a role in providing the first ray with adequate mobility and stability needed for performing activities of everyday life.1 According to the literature, nearly 50% of the trapezial fractures are a consequence of motorbike accidents,2 as we reported in our case.
Walker et al8 presented a classification based on the anatomic appearance of the fracture, which had no relationship to either treatment or prognosis. The fracture’s pattern - not mentioned on Walker’s classification - is the one of the most important differences from other published papers.
Associated fractures are reported in 80% of cases1 such as Bennett’s fracture, Rolando’s fracture, fractures of the scaphoid4,5 and distal radius fractures.3
Occasionally they may also be associated with ligament damage.6 The presented case had no associated injuries.
The clinical presentation can be quite variable depending on the displacement of the fracture and the involvement of the trapeziometacarpal joint. It could be minimal, with no gross deformity and almost full ROM of the thumb,9 like the presented case.
There is a high probability of misdiagnosing or missing these fractures in ED4 on account of their rarity and poor radiographic appearance on routine radiographs.5
Imaging consists of plain radiographs, but often undisplaced fractures can be imperceptible on these.4,6 Trapezial fractures diagnosis can be made by radiographs with specific projections4,5,9,10 such as Bett’s view (true lateral view of the trapeziometacarpal joint),1,3 Robert’s view (true anteroposterior view of the trapeziometacarpal joint) and carpal tunnel view.3,5 However, the sensibility of conventional plain radiographs is poor, varying from 18% to 67%.3 Thus, it is important to have a high clinical suspicion based on history and mechanism of injury.1,6
Even with the initial negative projection radiograph, an additional CT scan3,4,6,7,10 or an MRI should be done to rule out occult fractures. CT scan is helpful in finding out the amount of displacement and the size of the fragments.3
MRI has additional value in detecting soft tissue injuries such as ligament ruptures.1,4
Trapezium fractures are rare; this means there is lack of experience in treating those fractures.7 The literature reports several management options, and universal treatment protocol for trapezium fractures is not standardized.3,6 Non-displaced fractures with adequate alignment of articular surface can be treated non-operatively; operative treatment is indicated for: displaced fractures, avulsion ridge fractures (as these are associated with higher risk of symptomatic nonunion) and highly comminuted fractures in high demand patients.
Most frequent management and treatment are non-operative (thumb immobilization in a plaster or other metacarpal-finger types of immobilizations).2,6 The results of the conservative treatment range from successful to dismal.3 Operative treatment options include closed/open reduction and internal fixation.2,3,5,6,9,10 arthroscopy assisted internal fixation,2,3,6,10 external fixator,8 and fragment7 or trapezium excision.9 In our case, conservative treatment followed by physiotherapy played a major role to recover a normal painless ROM.
One of the main issues about our case was its inconclusive radiographs, highlighting that pain and swelling at carpal or the thumb after a motorcycle accident should never be underestimated and should lead the physician to think about the possibility of a trapezial fracture, and not just to other common carpal injuries.
Nowadays, the treatment of trapezium fractures is based on experience, but a standardized treatment protocol must be developed for future treatment.

