










Serviços Personalizados
Journal

Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
 Similares em
SciELO
Similares em
SciELO Compartilhar

 Permalink
PermalinkActa Obstétrica e Ginecológica Portuguesa
versão impressa ISSN 1646-5830
Acta Obstet Ginecol Port vol.12 no.3 Coimbra set. 2018
CASE REPORT/CASO CLÍNICO
Inguinal Schwannoma: case report of a difficult diagnosis
Schwannoma de Região Inguinal: relato de um caso de difícil diagnóstico
Gabriel Antonio Cabriott Dumbra*, Marcos Rogério Miqueletti**
FACERES Medical School
*Acadêmico de medicina da Faculdade de Medicina Faceres
**Ginecologia, Obstetrícia e Mastologia, Universidade São Francisco de Bragança Paulista. Ambulatório Médico de Especialidades de São José do Rio Preto, Faculdade de Medicina Faceres e Clínica privada.
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Shwannoma, a typically benign tumor predominant in the cranial pairs, is very rarely found in the inguinal region and poorly described among gynecological tumors. We report the case of a female patient with inguinal mass and the difficulties of the diagnosis of tumors in this region, showing the complexity and importance of the appropriate propaedeutic.
Keywords: Schwannoma; Neurilenom; Differential diagnosis; Gynecological surgery.
Introducion
Schwannoma is a typically benign tumor that originates from Schwann cells in the myelin sheath of nerves and rarely appears in pelvic or inguinal regions1-3. Its diagnosis and treatment are difficult and depend on a good clinical reasoning. The main objective of this study is to report the case of a 57-year-old female patient with a nodule in the left inguinal region near the vulva, who was referred for a gynecological consultation. The aim of this study is to evaluate the difficulties of the diagnosis, which was discovered to be a schwannoma after an anatomopathological examination, an extremely rare tumor in such region.
Clinical Case
A 57-year-old female patient, menarche at age 11 and surgical menopause at age 29 due to uterine myomatosis, without the use of Hormone Replacement Therapy. She attended the hospital with a complaint of a 2 cm nodule in inguinocrural region on the left, hardened, and adhered to deep and painless tissues for 20 days. At gynecological examination, vaginal touch and contralateral inguinal region showed no alterations, and there was also the absence of phlogistic signs in the affected region. She denied fever, dysuria, urinary disorders, weight loss or palpable subcutaneous nodules. Before the case, ultrasound of superficial structures, nuclear magnetic resonance (MRI) of the abdomen and pelvis, as well as fine needle aspiration (FNA) of the lesion and return for reassessment were requested. The initial diagnostic hypothesis was Lymph node or tumor.
The results were abdominal MRI without changes, no lymph nodes or liquid in the cavity; MR of the pelvis with absence of inguinal nodules, US of superficial structures presenting “Solid, heterogeneous nodule, regular contours in the subcutaneous cellular tissue, with discreet flow on Doppler = 1.7X1,2 cm, distant 0.2 cm of the skin. Lymph node?”; FNA with absence of malignant neoplastic cells - numerous neutrophils, lymphocytes and erythrocytes, discrete flow on Doppler.
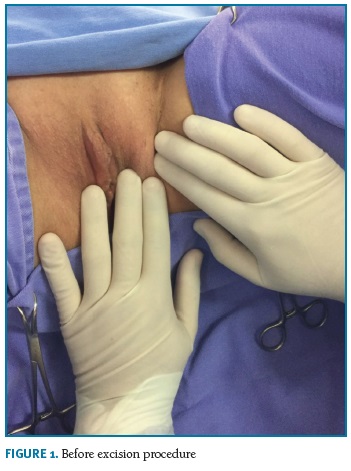
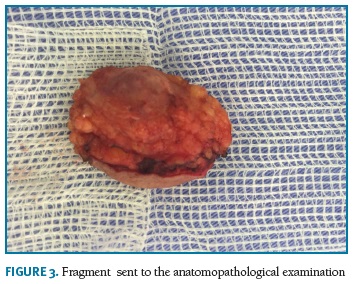
In view of the situation, the excision procedure of the nodule of unclarified etiology was taken (Figures 1 and 2), and the necessary preoperative examinations were requested. The results showed no alterations that would make the surgical procedure difficult. After surgery, a fragment was sent to the anatomopathological examination (Figure 3) with a diagnostic conclusion of Schwannoma (Neurilenoma).

Discussion
Schwannoma, previously known as Neurilenoma, appears predominantly in the cranial pairs in the spinal cord, being less frequent in the retroperitoneum, in the posterior mediastinum and in the pelvis. Other regions are considered rare, and there are no literature reports of this type of neoplasia in the inguinal region. These tumors are usually detected between the third and fifth decades of life, with an equal incidence in men and women2-5.
The skin lesion usually presents as a nodule, sessile-based, smooth surface, soft to palpation, variable size (1-3 cm on average), slow growth, and asymptomatic. Pain and tenderness may be present, especially in cases where tumor growth causes compression of the affected nerve and surrounding structures, and even paresthesia may occur6,7-9. Malignant transformation occurs in approximately 3-10% of the cases, presenting great cellular proliferation, atypical mitotic activity, cellular and nuclear pleomorphism and foci of necrosis, and a greater association with von Recklinghausen's disease3,6.
Based on the literature, the appropriate diagnostic procedure commonly uses computerized tomography (CT) as the first method. MRI, however, should always be the method of choice, although both do not often present conclusive alterations. One can attempt to diagnose the nature of the lesion through fine needle aspiration biopsy (FNAB)4,6. If this is not conclusive, the next procedure is resection of the nodule for evaluation by conventional anatomopathological examination, in order to determine tumor malignancy or benignity6.
After definitive diagnosis of benignity, the treatment of choice is surgery with excision of the tumor nodule, preserving or not the tumor's nerve, depending on its importance2,3,10-13. Tumor recurrence is low, and there is a significant association with the degree of mitotic count.
Despite the difficult diagnosis due to the rarity of the case, when the research methods and appropriate treatment measures are followed based on medical semiology, the objectives of the medical care are fulfilled regardless of the etiology. Also important is the anatomopathological examination for the unmistakable diagnosis.
REFERENCES
1. Armas Pérez BA, Fontes Maestri MC, Rubino de la Rosa J, Reyes Balseiro ES, Armas Moredo K. Schwannoma benigno de mediastino: a propósito de un caso. Rev Cubana Cir [serie en Internet]. 2008 Jul-Sep. 47(3). [Citado 2011 Feb 04] http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0034-74932008000300010 &lng=es. [ Links ]
2. Harjula A, Mttila S, Luosto R, Kostiainen S, Mattila I. Medistinal neurogenic tumours. Scand J Thor Cardiovasc Surg 1986; 20: 115-118. [ Links ]
3. Fletcher CDM, Davies SE, Mvkee PH. Cellular schwannoma: a distinct pseudosarcomatous entity.Histopathology 1987;11:21-35. [ Links ]
4. Dahl I, Hagmar B, Idvall I. Benign solitary neurilemoma (schwannoma). Acta Pathol Microbiol Immunol Scand 1984; 91: 91-101. [ Links ]
5. Rosai J. Tumours of the soft tissue. Ackerman's surgical pathology. 2nd ed. New York, Mosby, 1996; 2.042-5. [ Links ]
6. Sardinha SDCS, Paza AO, Vargas PA, Moreira RWF, De Moraes M. Schwannoma of the oral cavity. Histological and immunohistochemical features. Braz J Oral Sci. 2005;4 (14):806-809. [ Links ]
7. Casadei GP, Scheithauer BW, Hirose T et al. Cellular schwannomna: a clinicopathologic, DNA flow cytometric, and proliferation marker of 70 patients. Cancer 1995; 75(5): 1.109-119. [ Links ]
8. Patil K, Mahima VG , Srikanth HS, Saikrishna D. Central schwannoma of mandible. Jomfp. 2009;13(1):23-26. [ Links ]
9. Bansal R, Trivedi P, Patel S. Schwannoma of the tongue. Oral Oncology Extra. 2005;41(7):15-17. [ Links ]
10. Kanatas A, Mucke T, Houghton D, Mitchell DA. Schwannomas of the head and neck. Oncol Rev. 2009;3(2):107-11.14. [ Links ]
11. Nascimento GJ, Albuquerque PRD, Galvão HC, Lisboa LCA, Souza LB. 38-year review of oral schwannomas and neurofibromas in a Brazilian population: clinical, histopathological and immunohistochemical study. Clin Oral Investig. 2011;15(3):329-35. [ Links ] Epub 2010 Mar 9.]
12. Urakawa T, Kawakita N, Nagahata Y. A case of benign schwannoma of the thoracic wall mimicking a malignant tumor. Kobe J Med Sci 1993; 39: 123-13l. [ Links ]
13. Ball JHS, Sonnendecker EW, Sevitz H et al. - Retroperitoneal malignant schwannoma. A case report. S Afr Med J, 1987, 71(1):49-52. [ Links ]
14.Murray RJ, Criner GJ, Siegel E. Multiple schwannomas presenting as a mass of the lateral chest wall. AJR1988; 151: 1.250-251. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Gabriel Antonio Cabriott Dumbra
Rua José Francisco Vitorel nº 55, apto62A, Bairro Vila Imperial
São José do Rio Preto- São Paulo, Brasil. CEP 15015-515.
E-Mail: gabriel_dumbra@hotmail.com
Recebido em: 22/10/2017
Aceite para publicação: 20/11/2017

