










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkAngiologia e Cirurgia Vascular
versão impressa ISSN 1646-706X
Angiol Cir Vasc vol.16 no.3 Lisboa set. 2020
CLINICAL CASE
Internal carotid pseudoaneurysm caused by migration of a coronary guidewire fragment: a case of a broken arrow
Pseudoaneurisma da artéria catótida interna causado por migração de fragmento de fio-guia coronário
Nuno Henriques Coelho1, Pedro Monteiro1, Rita Augusto1, Evelise Pinto1, Carolina Semião1, João Ribeiro1, João Peixoto1, Luís Fernandes1, Ricardo Gouveia1, Victor Martins1, Alexandra Canedo1
1 Centro Hospitalar de Vila Nova de Gaia/Espinho, Serviço de Angiologia e Cirurgia Vascular
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Introduction: Guidewire fracture is a rare complication of percutaneous coronary intervention (PCI). Retained fragments can cause thrombosis, dissection, perforation of the vessel or embolize. When is impossible to withdraw or to trap the fragment during the procedure, management is debatable between surgical removal or conservative approach. When choosing to leave the fragment in place, the patient remains at risk for all of the aforementioned complications.
Clinical Case: 65-year-old male patient submitted to PCI with stenting of distal right coronary artery in 2017. A proximal optimization technique was performed, with a guidewire placed in the posterior descending artery (PDA). After stenting, the protection guidewire became entrapped and after several retrieval attempts, it fractured. Wire fragment remained within the RCA and ascending aorta with a free mobile distal part in the beginning of the innominate artery. Multiple attempts went in vain for wire retrieval and a conservative approach was adopted. Two and a half years later, the patient felt a sudden chest pain and then collapsed. He was transferred to our Hospital for emergent surgery due to cardiac tamponade. Intra-operatively, cardiac surgeons found the guidewire perforating the posterior descending artery. When trying to pull it out, the guidewire fractured again. Post-intervention CTA revealed migration of the fragmented guidewire now it was entrapped in a tortuous initial portion of the right internal carotid artery and a small pseudoaneurysm was visible at the distal portion of the wire. Surgical approach was performed revealing the presence of the wire within the carotid medial wall, in a subintimal plane. The 7 cm fragment was successfully withdrawn, through a common carotid transverse incision. Pseudoaneurismectomy was performed and carotid artery bifurcation reconstruction with internal carotid artery re-implantation into the bifurcation, end-to-end anastomosis. The patient had an uneventful postoperative course.
Conclusion: Although leaving the wire in place remains an option, coronary guidewire fractured fragments can be associated not only with immediate complications but also with potential adverse events in the long run.
Keywords: Percutaneous coronary intervention complications; broken guidewire; guidewire embolization; foreign body in ascending aorta; cardiac tamponade; internal carotid pseudoaneurysm
RESUMO
Introdução: A fratura do fio-guia durante uma intervenção coronária percutânea (ICP) é uma complicação rara. Os fragmentos retidos podem provocar trombose, disseção ou perfuração do vaso ou até mesmo embolizar para outros territórios. Quando é impossível recuperar ou aprisionar o fragmento durante o procedimento inicial, a abordagem seguinte é questionável entre uma remoção cirúrgica ou uma abordagem mais conservadora. Quando a segunda opção é a escolhida, a eventualidade de ocorrência de qualquer uma das complicações acima referidas mantém-se.
Caso Clínico: Doente de 65 anos, submetido a ICP com stenting da coronária direita (ACD) em 2017. Para tal foi utilizada uma proximal optimization technique, com colocação de fio-guia na descendente posterior (ADP). Após o stenting, o fio de proteção ficou preso e após várias tentativas de remoção acabou por fraturar. O fragmento encontrava-se ao longo do interior da ACD e aorta ascendente, com a sua porção proximal localizada a nível do tronco arterial braquiocefálico. Múltiplas tentativas de remoção endovascular foram tentadas em vão, optando-se por uma estratégia conservadora. Dois anos e meio depois, o doente sente uma precordialgia aguda, acabando por colapsar. É transferido para a nossa Instituição onde é submetido a cirurgia cardíaca urgente. Intra-operatoriamente é constatada a presença do fragmento do fio-guia a perfurar a ADP. Este mesmo fragmento, ao ser puxado na tentativa de ser recuperado, volta a fraturar. O angioTC pós-intervenção revelou uma migração cefálica do restante fragmento agora encontrando-se retido na artéria carótida comum e porção inicial da artéria carótida interna direitas, visualizando-se um falso aneurisma a nível da extremidade distal do fragmento. O doente foi submetido a cirurgia carotídea, recuperando-se o fragmento através de uma incisão transversal da artéria carótida comum. Foi realizada pseudoaneurismectomia, com reimplantação da artéria carótida interna na bifurcação carotídea através de uma anastomose topo-a-topo. O pós-operatório decorreu sem complicações.
Conclusão: Apesar de o tratamento conservador poder ser uma opção, os fragmentos secundários a fratura de fio-guia podem associar-se não só a complicações imediatas como também a complicações associadas a risco de vida a longo prazo, tal como demonstrado neste caso.
Palavras-chave: Complicações da intervenção coronária percutânea; fratura de fio-guia; migração de fio-guia; tamponamento cardíaco; pseudoaneurisma da carótida interna
Introduction
Coronary guidewire entrapment and fracture is a rare, yet feared complication of percutaneous coronary intervention (PCI). It represents an important technical challenge having a described incidence of 0,2 to 0,8%.(1-4) Nevertheless, with the current frequency of more complex and demanding interventions (i.e. addressing chronic total occlusions (CTOs), heavily calcified or tortuous vessels and bifurcation lesions) the incidence might be higher than previously reported.(5) Guidewire remnants may lead to life-threatening complications such as intracoronary thrombosis and consequent infarction, vessel perforation with associated cardiac tamponade or systemic embolization.(4) Guidewire retrieval is highly recommended during the index procedure, preferably using percutaneous methods.(6) When it is impossible to withdraw or to trap the fragment percutaneously, management ranges from conservative to surgical removal depending on the location, chronicity and clinical condition of the patient. However, when leaving the wire in place, the patient remains at risk for all of the aforementioned complications. We describe a case of this uncommon complication in which an entrapped guidewire induced a cardiac tamponade and a carotid pseudoaneurysm 2,5 years after PCI, requiring a successful emergent surgical intervention.
Case report
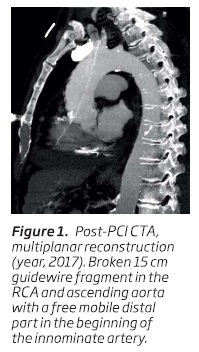
A 65-year-old man underwent PCI due to low threshold angina in 2017, in another Hospital. PCI description highlighted a severe distal right coronary artery (RCA) stenosis. A proximal optimization technique (POT) was performed with a balance middle weight guidewire (BMW, Abbott-Vascular, Santa Clara, CA) placed in the posterior descending artery (PDA). After stenting, the protection PDA guidewire became “jailed” between the deployed stent and the severely calcified vessel wall. After several pullback maneuvers it broke leaving a fragment of approximately 15 cm length in place. Multiple attempts (snare catheter, two-wire rotation technique) went in vain for wire removal. The patient was clinically stable and considering that the risk of further aggressive manipulation could outweigh the benefits it was decided to end the procedure. Post-interventional computed tomography angiography (CTA) revealed the broken guidewire in the RCA and ascending aorta with a free mobile distal part in the beginning of the innominate artery (figure 1).
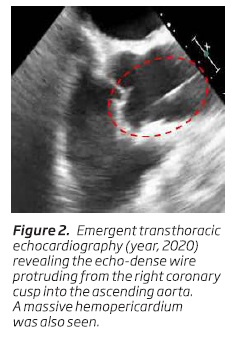
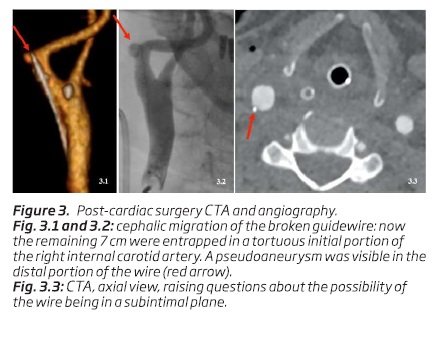
Although informed about the risks of leaving the wire in place, the patient refused surgical intervention. He underwent a regular follow-up program during which he did not experienced any cardiovascular symptom or shown any deterioration in his left ventricular ejection. Two and a half years later, the patient felt a sudden chest pain and then collapsed. Emergent transthoracic echocardiography revealed the echo-dense wire protruding from the coronary cusp into the ascending aorta and a massive hemopericardium (figure 2).After pericardiocentesis he was transferred to our Institution for emergent cardiac surgery. Intra-operatively, cardiac surgeons found the guidewire fragment perforating the PDA. When pulling the fragment out, it fractured again and only about 8 cm of the distal portion of the wire were recovered. Transesophageal echocardiography no longer demonstrated the wire in the ascending aorta as seen in the beginning of the procedure. After cardiac surgery and hemodynamic stabilization, a CTA was performed revealing a cephalic migration of fragment: now it was entrapped in a tortuous initial portion of the right internal carotid artery and a small pseudoaneurysm was visible at the distal portion of the wire (figure 3.1 and 3.2). CTA axial views suggested that the fragment might be in a subintimal plane (figure 3.3).
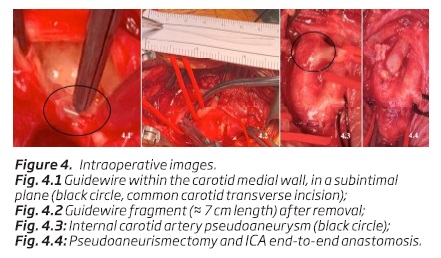
A common carotid transverse incision revealed the presence of the wire within the carotid medial wall, in a subintimal plane and the remnant 7 cm fragment was finally withdrawn (figure 4.1 and 4.2). Internal carotid redundancy allowed successful performance of pseudoaneurismectomy and internal carotid artery re-implantation into the bifurcation, with an end-to-end anastomosis (figure 4.3 and 4.4). Patient had an uneventful postoperative course without any signs of perioperative or postoperative myocardial infarction or cerebrovascular events, being discharged at the eight postoperative day. He has now 6 months follow up, without any complications.
Discussion
Our case demonstrates two potential life-threatening consequences of guidewire entrapment and fracture during PCI: coronary perforation with associated cardiac tamponade and fragment embolization. On the one hand, there is a growing number of complex procedures that require advanced operator skills and use of multiple coronary armamentarium have a greater risk of this event. On the other hand, probably only a small portion of cases are reported. So, this PCI complication is clearly underestimated.(7) Besides the coronary lesion, a combination of factors like guidewire entrapment in the subintimal space, over-rotation and guidewire “jailing” techniques can lead to this unfortunate event. Typically, the breaking point is at the junction of the hydrophilic coated part and the non-hydrophilic one leading to detachment of a short fragment that most of the time can be entrapped in distal coronary branches.(5) In the present case, the breaking point was at the core of the wire leaving a lengthy 15 cm fragment in place. Besides lesion characteristics and the employed revascularization techniques a structural failure of the wire may also have played a role. In the presence of such a lengthy fragment, resistant to all the techniques employed to retrieve it, the risks and benefits of aggressive measures to withdraw it must be weighed. Extensive manipulation during repeated attempts can lead to potentially catastrophic consequences (coronary dissection, rupture or thrombosis).(1,2) Patient condition, location and size of the remnant should be considered. Although small fragments located in terminal and small vessels can be left in situ without complications(5,8-10) large remnants located in the ascending aorta as in this case carry a high risk of valvular damage, wall penetration even cerebral embolization.(11,7,12) So, the decision to end the procedure and propose surgical removal surgery had these factors into account. The informed decision of the patient not to undergo surgery for wire retrieval put him in danger for future complications. When presenting in cardiac shock, surgical interventions for wire retrieval carry a mortality of nearly 40%.(3)When cardiac surgeons pulled the wire fragment it worked as a bow and arrow mechanism leading to another fragment which suffered a cephalic migration stopped only by internal carotid tortuosity. It was difficult to be sure about the subintimal location of the wire only by CTA. The common carotid transverse incision allowed fast control and easy retrieval of the wire fragment. The pseudoaneurysm was the other issue to resolve and several repair techniques were considered (patch angioplasty, interposition graft, end-to-end anastomosis). After further ICA dissection, we were able to take advantage of its redundancy. It allowed us to perform an end-to-end anastomosis, after pseudoaneurysm exclusion, using only autologous tissue. In the current era of increasing numbers of PCI procedures, the incidence of entrapped or retained coronary armamentarium will rise. As the present case demonstrates, not only cardiologists and cardiothoracic surgeons will be involved. When systemic embolization occurs, vascular surgeons have also an important role to play and inventive endovascular and surgical solutions are required.
Conclusion
In the case of fractured guidewire during PCI, leaving the wire in place remains an option. Nevertheless, guidewire fragments can be associated not only with immediate complications but also with potential complications in the long run. This unusual case, demonstrates a late life-threatening complication which required a multidisciplinary approach to prevent this “broken arrow” do produce more damages.
REFERENCES
1. Shahid M Khan, David W Ho, Temujin Dinaram, Jason M Lazar, J. D. M. Conservative management of broken guidewire: Case reports. SAGE Open Med. Case Reports (2014). DOI: 10.1177/2050313X14554478 [ Links ]
2. Danek, B. A., Karatasakis, A. & Brilakis, E. S. Consequences and treatment of guidewire entrapment and fracture during percutaneous coronary intervention. Cardiovasc. Revascularization Med. 1-5 (2016). DOI: 10.1016/j.carrev.2015.12.005 [ Links ]
3. Idhrees, A. M., Radhakrishnan, B. K., Panicker, T., Pillai, V. & Karunakaran, J. Entrapment of guidewire in left anterior descending artery: Surgical management. Asian Cardiovasc. Thorac. Ann. 0, 1-2 (2016). [ Links ]
4. Ahmad, T., Chithiraichelvan, S., Patil, T. A. & Jawali, V. Surgical retrieval of entrapped coronary angioplasty guidewire from the aorta. Asian Cardiovasc. Thorac. Ann. 24, 81-84 (2016). [ Links ]
5. Danek, B. A., Karatasakis, A. & Brilakis, E. S. Cardiovascular Revascularization Medicine Consequences and treatment of guidewire entrapment and fracture during percutaneous coronary intervention. Cardiovasc. Revascularization Med. 1-5 (2016). DOI: 10.1016/j.carrev.2015.12.005 [ Links ]
6. Capuano, F., Simon, C., Roscitano, A. & Sinatra, R. Percutaneous transluminal coronary angioplasty hardware entrapment: guidewire entrapment. J Cardiovasc Med 9, 1140-1141 (2008). [ Links ]
7. Domaradzki, W., Sanetra, K., Skwarna, B. & Jankowska-sanetra, J. Surgical retrieval of entrapped coronary guidewire remnant: 3-year angiographic evaluation. kardiochirurgia i Torakochirurgia 15, 4-7 (2018). [ Links ]
8. Valery Meledin, Vladimir Perkhulov, Gera Gandelman, Jacob George, S. S. Fractured Guidewire Entrapped in the Ostium of Right Coronary Artery Mimicking Aortic Flap. JACC Cardiovasc. Interv. 12, 12-13 (2019). [ Links ]
9. Stefan Baumanna, Daniel Rupp, Tobias Bechera, Michael Behnesa, Maliha Sadick, Martin Borggrefe, I. A. Retrieval of a fractured angioplasty guidewire after percutaneous retrograde revascularization of coronary chronic total occlusion. Coron. Artery Dis. 10-11 (2017). DOI: 10.1097/MCA.0000000000000535 [ Links ]
10. Koulouris S, S. M. An unusual case of an angioplasty wire entrapped and fractured within the struts of a recently implanted coronary stent: Treatment with the implantation of a “jailing” stent. Hell. J. Cardiol. 10-12 (2017). DOI: 10.1016/j.hjc.2017.03.012
11. Yildiz BS, et al. Retrieval of a fractured guidewire with balloon support in intermediate coronary artery: A rare complication and management. Indian Hear. J. 10-12 (2016). DOI: 10.1016/j.ihj.2016.02.012 [ Links ]
12. Aranzulla, T. C. One, two, three … breakdance and twist. Catheter Cardiovasc Interv. 1-8 (2019). DOI: 10.1002/ccd.28643 [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Correio eletrónico: nunoc.90@gmail.com (N. Coelho).
Recebido a 03 de agosto de 2020. Aceite a 15 de setembro de 2020.

