











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
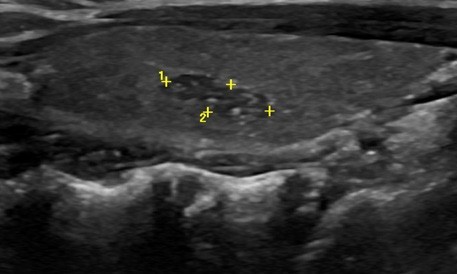
We present a case of a pediatric patient with history of recurrent episodes of tonsillitis since 2 years of age. In the context of infectious mononucleosis, a cervical ultrasound was performed, which revealed a relatively hypoechoic lesion in the right lobe of the thyroid gland, similar to normal thymus echogenicity (Fig. 1). Thyroid function tests: TT3 (total triiodothyronine), TT4 (total tetraiodothyronine), FT3 (free triiodothyronine), FT4 (free tetraiodothyronine) and TSH (thyroid-stimulating hormone) were normal. After 3 years of follow-up, the intrathyroidal nodule maintained the same characteristics, having decreased in size from 12 mm to 8 mm (Fig. 2). Decision of conservative management with strict monitoring until involution was taken, along with parents’ consent.
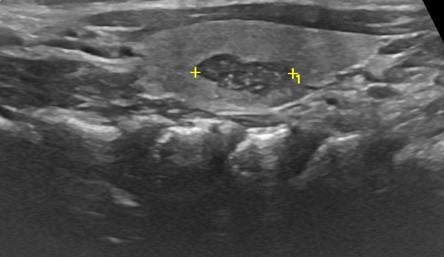
Figure 1: Ultrasound showing a relatively hypoechoic 12mm lesion in the right lobe of the thyroid gland, with sharp margins and multiple echogenic foci, similar to thymus tissue.
Role of ultrasound in diagnosis and follow up of the ectopic thymus
As ultrasound is of common use nowadays, the number of incidental lesions found is increasingly high, including simple cysts or hypoechoic nodules, such as ectopic thymus. Ectopic thymus is a well-known embryological abnormality in children, despite being considered rare. It is most frequently found in the cervical area or mediastinum, yet rarely in the pericardium, hilar area, chest wall or axilla. Ectopic intrathyroidal thymic tissue is also rare.1
Normal thymus tissue, located in the superior and anterior compartments of the mediastinum, develops from the endoderm of the third and fourth pharyngeal pouches. Thymic parenchyma in children has a characteristic ultrasound appearance, with fusiform shape, well-defined margins and echogenicity between the thyroid gland and the surrounding muscle. Furthermore, it has multiple echogenic foci, portraying a “starry sky” appearance. This distinctive feature is created by overlapped fat and lymphoid tissue.2 So, if an intrathyroidal lesion has sharp margins and echotexture similar to the thymus, with no abnormal echogenicities in the surrounding thyroid area,as well as no abnormal lymph nodes, it requires no further action. Only sonographic follow-up is advised, since thymic tissue may automatically degrade and contract. However, if the diagnosis is uncertain, based on sonographic features, or if the mass has suspicious characteristics, further investigation, including ultrasound-guided fine-needle aspiration or additional imaging should be performed.3
In conclusion, it is important to identify and to be aware of thymic rests and their normal sonographic appearance, so that they won’t be confused with other neoplastic thyroid masses, therefore avoiding unnecessary anxiety and intervention, especially in the pediatric population.

